

Head Injury and Long-term Mortality Risk in Community-Dwelling Adults
- PMID: 36689218
- PMCID: PMC9871946
- DOI: 10.1001/jamaneurol.2022.5024
Head Injury and Long-term Mortality Risk in Community-Dwelling Adults
Abstract
Importance: Head injury is associated with significant short-term morbidity and mortality. Research regarding the implications of head injury for long-term survival in community-dwelling adults remains limited.
Objective: To evaluate the association of head injury with long-term all-cause mortality risk among community-dwelling adults, with consideration of head injury frequency and severity.
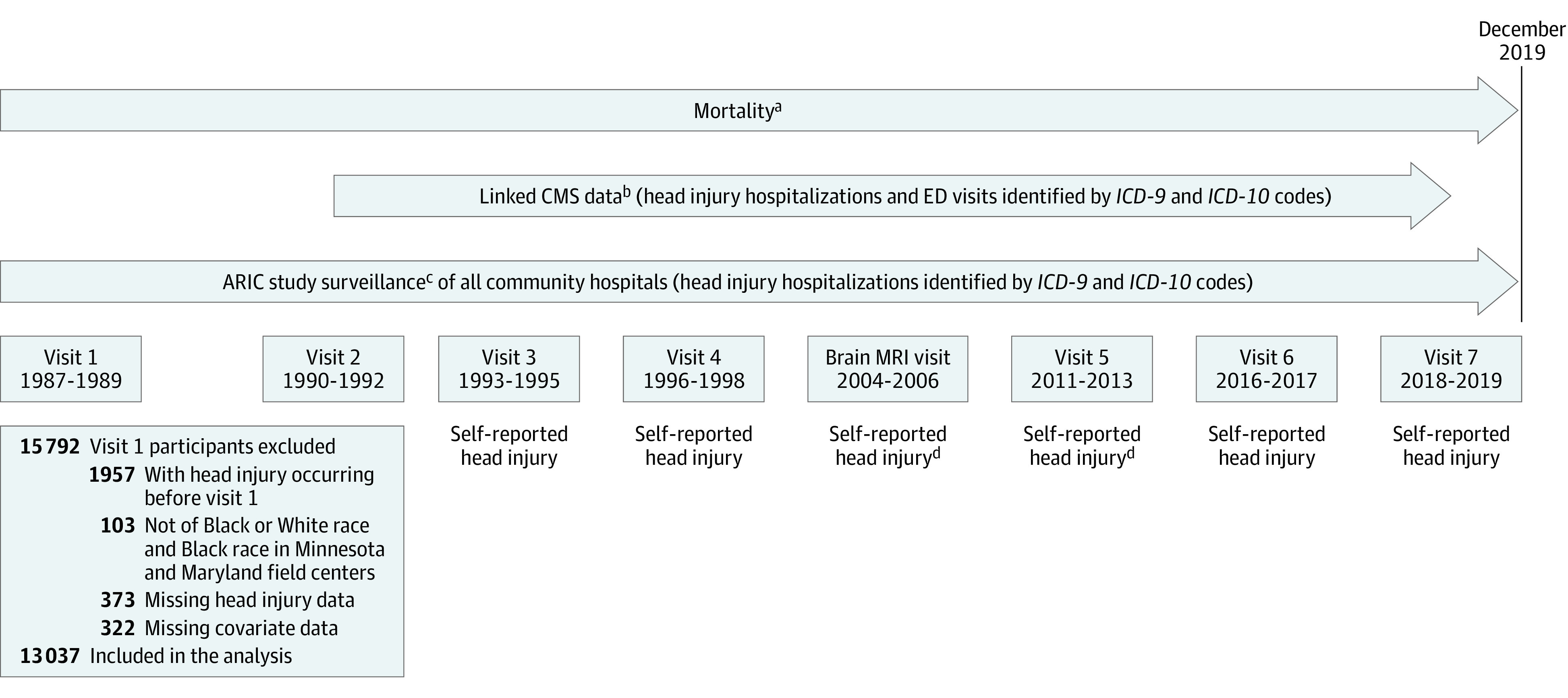
Design, setting, and participants: This cohort study included participants with and without head injury in the Atherosclerosis Risk in Communities (ARIC) study, an ongoing prospective cohort study with follow-up from 1987 through 2019 in 4 US communities in Minnesota, Maryland, North Carolina, and Mississippi. Of 15 792 ARIC participants initially enrolled, 1957 were ineligible due to self-reported head injury at baseline; 103 participants not of Black or White race and Black participants at the Minnesota and Maryland field centers were excluded due to race-site aliasing; and an additional 695 participants with missing head injury date or covariate data were excluded, resulting in 13 037 eligible participants.
Exposures: Head injury frequency and severity, as defined via self-report in response to interview questions and via hospital-based International Classification of Diseases diagnostic codes (with head injury severity defined in the subset of head injury cases identified using these codes). Head injury was analyzed as a time-varying exposure.
Main outcomes and measures: All-cause mortality was ascertained via linkage to the National Death Index. Data were analyzed between August 5, 2021, and October 23, 2022.
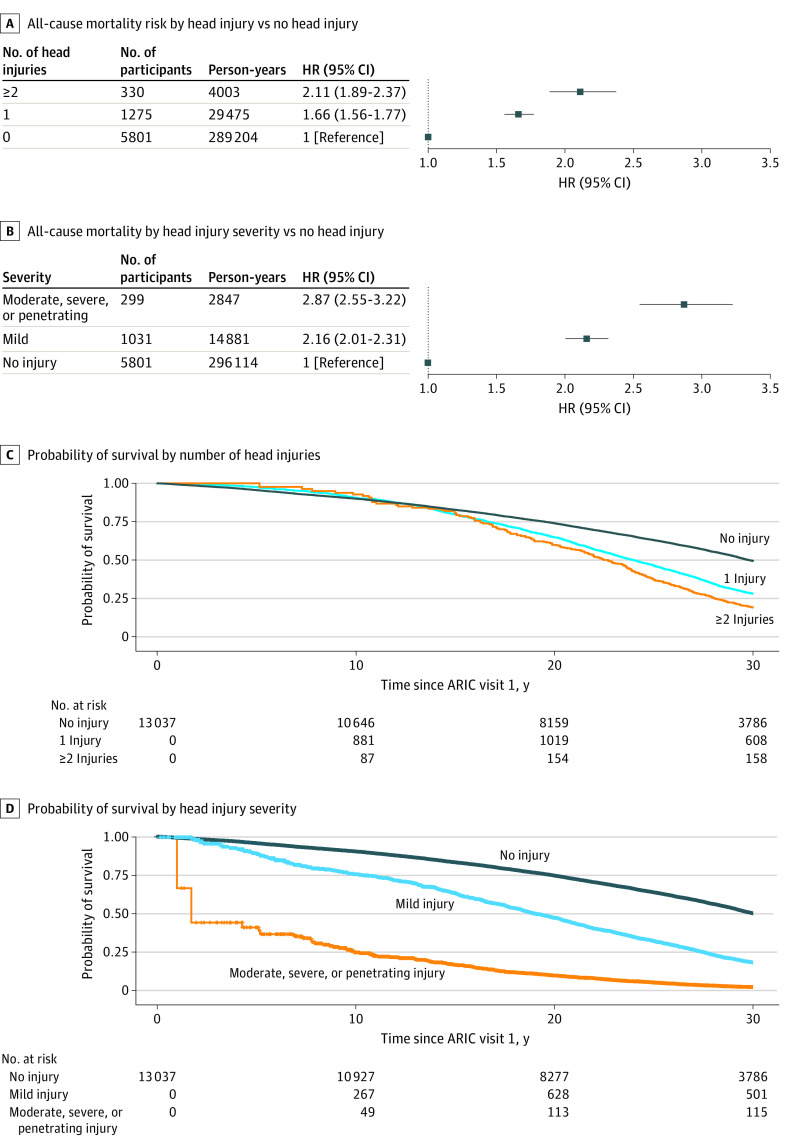
Results: More than one-half of participants were female (57.7%; 42.3% men), 27.9% were Black (72.1% White), and the median age at baseline was 54 years (IQR, 49-59 years). Median follow-up time was 27.0 years (IQR, 17.6-30.5 years). Head injuries occurred among 2402 participants (18.4%), most of which were classified as mild. The hazard ratio (HR) for all-cause mortality among individuals with head injury was 1.99 (95% CI, 1.88-2.11) compared with those with no head injury, with evidence of a dose-dependent association with head injury frequency (1 head injury: HR, 1.66 [95% CI, 1.56-1.77]; 2 or more head injuries: HR, 2.11 [95% CI, 1.89-2.37]) and severity (mild: HR, 2.16 [95% CI, 2.01-2.31]; moderate, severe, or penetrating: HR, 2.87 [95% CI, 2.55-3.22]). Estimates were similar by sex and race, with attenuated associations among individuals aged 54 years or older at baseline.
Conclusions and relevance: In this community-based cohort with more than 3 decades of longitudinal follow-up, head injury was associated with decreased long-term survival time in a dose-dependent manner, underscoring the importance of measures aimed at prevention and clinical interventions to reduce morbidity and mortality due to head injury.
Conflict of interest statement
Figures
References
-
- Menon DK, Schwab K, Wright DW, Maas AI; Demographics and Clinical Assessment Working Group of the International and Interagency Initiative toward Common Data Elements for Research on Traumatic Brain Injury and Psychological Health . Position statement: definition of traumatic brain injury. Arch Phys Med Rehabil. 2010;91(11):1637-1640. doi:10.1016/j.apmr.2010.05.017 - DOI - PubMed
-
- National Institute of Neurological Disorders and Stroke. Traumatic brain injury. Published 2022. Accessed May 1, 2022. https://www.ninds.nih.gov/health-information/disorders/traumatic-brain-i...
-
- Peterson AB, Thomas KE, Zhou H. Traumatic brain injury-related hospitalizations and deaths by age group, sex, and mechanism of injury: United States 2018 and 2019. Centers for Disease Control and Prevention; 2022.
-
- CDC WONDER. Centers for Disease Control and Prevention . Published 2022. Accessed October 1, 2022. https://wonder.cdc.gov
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
