

Disparities in Wait Times for Care Among US Veterans by Race and Ethnicity
- PMID: 36689224
- PMCID: PMC9871804
- DOI: 10.1001/jamanetworkopen.2022.52061
Disparities in Wait Times for Care Among US Veterans by Race and Ethnicity
Abstract
Importance: Prior studies indicate that Black and Hispanic vs White veterans wait longer for care. However, these studies do not capture the COVID-19 pandemic, which caused care access disruptions, nor implementation of the US Department of Veterans Affairs (VA) Maintaining Internal Systems and Strengthening Integrated Outside Networks Act (MISSION), which is intended to improve care access by increasing veterans' options to use community clinicians.
Objective: To determine whether wait times increased differentially for Black and Hispanic compared with White veterans from the pre-COVID-19 to COVID-19 periods given concurrent MISSION implementation.
Design, setting, and participants: This cross-sectional study used data from the VA's Corporate Data Warehouse for fiscal years 2019 to 2021 (October 1, 2018, to September 30, 2021). Participants included Black, Hispanic, and White veterans with a new consultation for outpatient cardiology and/or orthopedic services during the study period. Multivariable mixed-effects models were used to estimate individual-level adjusted wait times and a likelihood ratio test of the significance of wait time disparity change over time.
Main outcomes and measures: Overall mean wait times and facility-level adjusted relative mean wait time ratios.
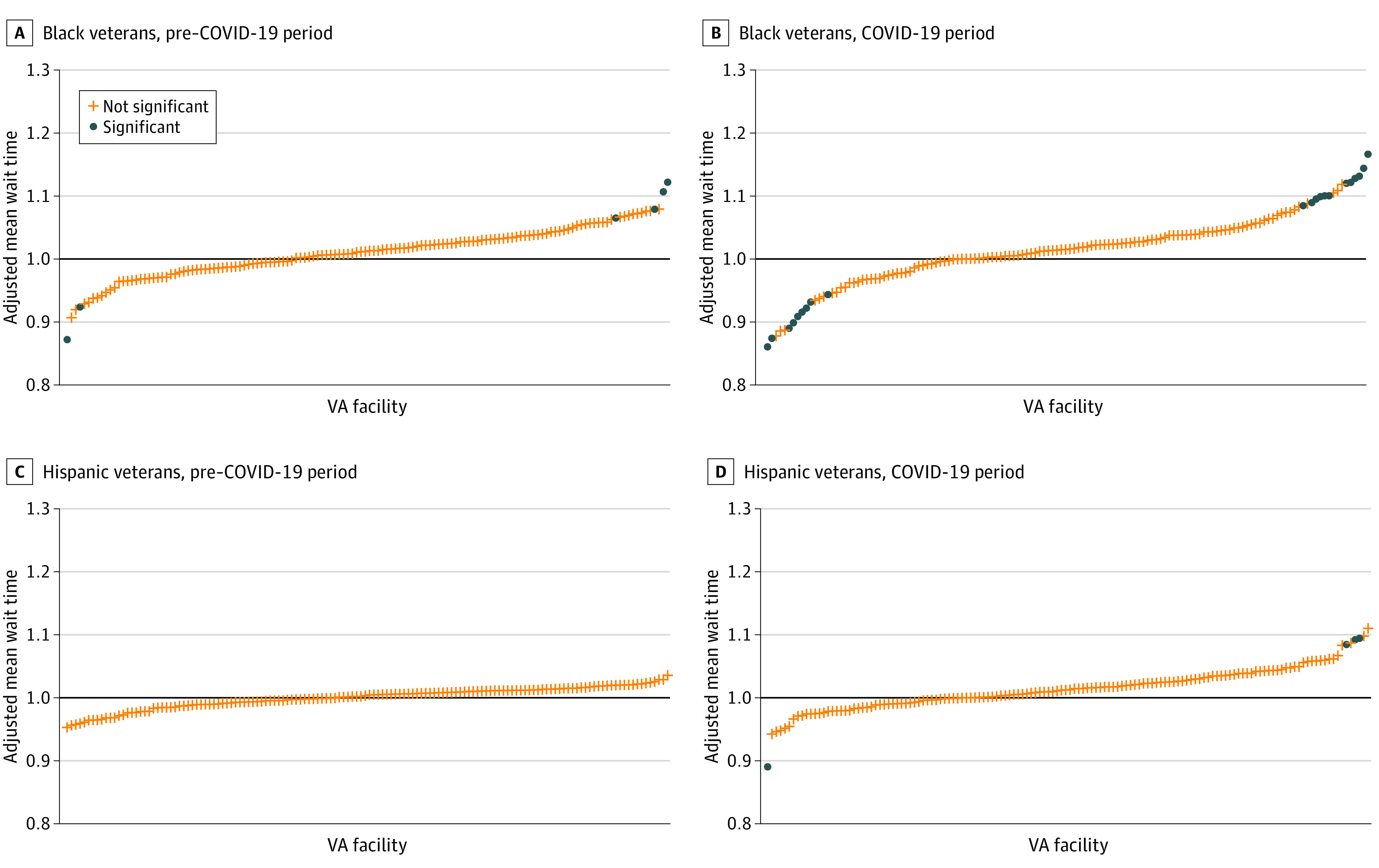
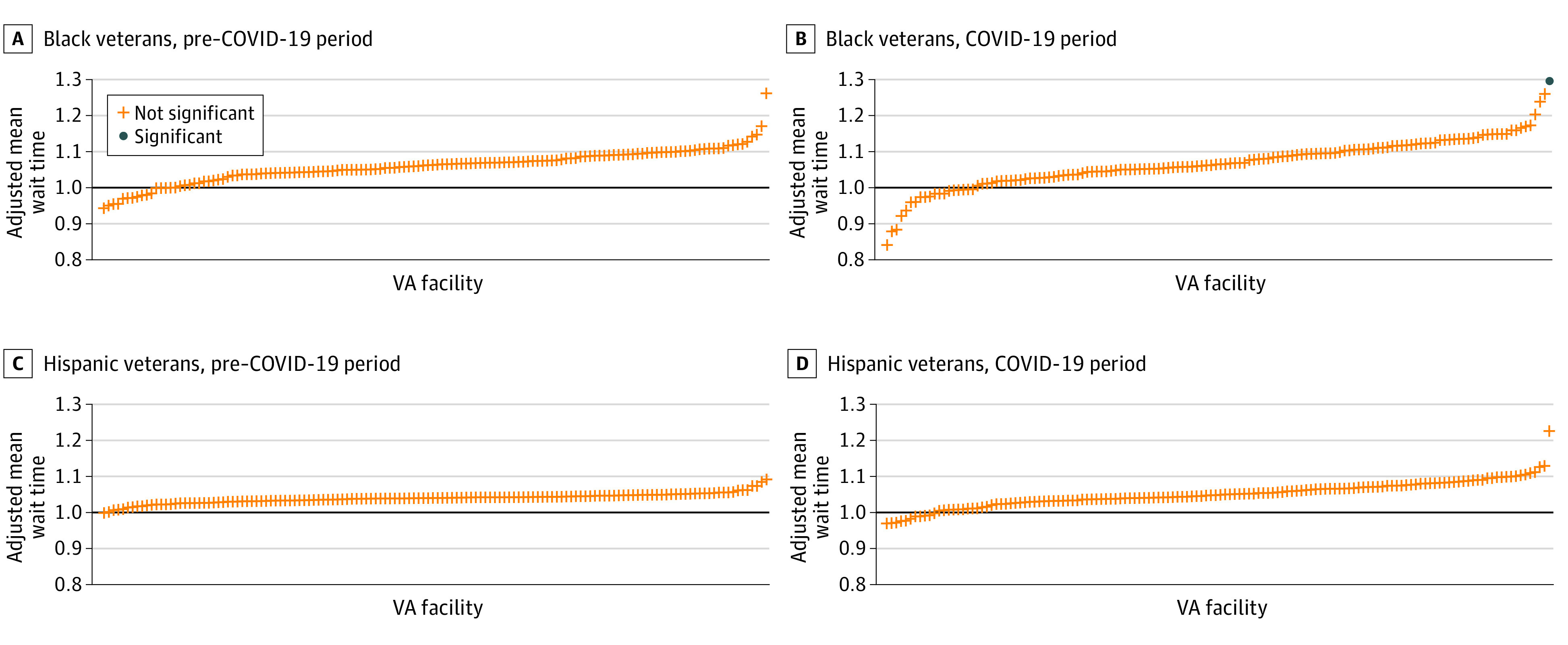
Results: The study included 1 162 148 veterans (mean [SD] age, 63.4 [14.4] years; 80.8% men). Significant wait time disparities were evident for orthopedic services (eg, Black veterans had wait times 2.09 [95% CI, 1.57-2.61] days longer than those for White veterans) in the pre-COVID-19 period, but not for cardiology services. Mean wait times increased from the pre-COVID-19 to COVID-19 periods for both services for all 3 racial and ethnic groups (eg, Hispanic wait times for cardiology services increased 5.09 [95% CI, 3.62-6.55] days). Wait time disparities for Black veterans (4.10 [95% CI, 2.44-5.19] days) and Hispanic veterans (4.40 [95% CI, 2.76-6.05] days) vs White veterans (3.75 [95% CI, 2.30-5.19] days) increased significantly from the pre-COVID-19 to COVID-19 periods (P < .001). During the COVID-19 period, significant disparities were evident for orthopedic services (eg, mean wait times for Hispanic vs White veterans were 1.98 [95% CI, 1.32-2.64] days longer) but not for cardiology services. Although there was variation in wait time ratios across the 140 facilities, only 6 facility wait time ratios were significant during the pre-COVID-19 period and 26 during the COVID-19 period.
Conclusions and relevance: These findings suggest that wait time disparities increased from the pre-COVID-19 to COVID-19 periods, especially for orthopedic services for both Black and Hispanic veterans, despite MISSION's goal to improve access. Facility-level analyses identified potential sites that could be targeted to reduce disparities.
Conflict of interest statement
Figures
Similar articles
-
Racial and Ethnic and Rural Variations in Access to Primary Care for Veterans Following the MISSION Act.JAMA Health Forum. 2024 Jun 7;5(6):e241568. doi: 10.1001/jamahealthforum.2024.1568. JAMA Health Forum. 2024. PMID: 38904952 Free PMC article.
-
Using the Kitagawa Decomposition to Measure Overall-and Individual Facility Contributions to-Within-facility and Between-facility Differences: Analyzing Racial and Ethnic Wait Time Disparities in the Veterans Health Administration.Med Care. 2023 Jun 1;61(6):392-399. doi: 10.1097/MLR.0000000000001849. Epub 2023 Apr 17. Med Care. 2023. PMID: 37068035 Free PMC article.
-
Geographic Variation in Appointment Wait Times for US Military Veterans.JAMA Netw Open. 2022 Aug 1;5(8):e2228783. doi: 10.1001/jamanetworkopen.2022.28783. JAMA Netw Open. 2022. PMID: 36006640 Free PMC article.
-
Mortality Disparities in Racial/Ethnic Minority Groups in the Veterans Health Administration: An Evidence Review and Map.Am J Public Health. 2018 Mar;108(3):e1-e11. doi: 10.2105/AJPH.2017.304246. Am J Public Health. 2018. PMID: 29412713 Free PMC article. Review.
-
Interventions to Improve Minority Health Care and Reduce Racial and Ethnic Disparities [Internet].Washington (DC): Department of Veterans Affairs (US); 2011 Sep. Washington (DC): Department of Veterans Affairs (US); 2011 Sep. PMID: 22206109 Free Books & Documents. Review.
Cited by
-
Racial and Ethnic and Rural Variations in Access to Primary Care for Veterans Following the MISSION Act.JAMA Health Forum. 2024 Jun 7;5(6):e241568. doi: 10.1001/jamahealthforum.2024.1568. JAMA Health Forum. 2024. PMID: 38904952 Free PMC article.
-
Health Equity in the Veterans Health Administration From Veterans' Perspectives by Race and Sex.JAMA Netw Open. 2024 Feb 5;7(2):e2356600. doi: 10.1001/jamanetworkopen.2023.56600. JAMA Netw Open. 2024. PMID: 38373000 Free PMC article.
-
Joint Efforts: A Review of Large Joint and Bursa Steroid Injections and Aspirations by Primary Care Physicians.J Gen Intern Med. 2025 Apr 17. doi: 10.1007/s11606-025-09490-x. Online ahead of print. J Gen Intern Med. 2025. PMID: 40246753 Review.
-
Implementation of a Dedicated Intake Team Reduces Time to Massed PTSD Treatment.J Behav Health Serv Res. 2025 Apr;52(2):342-356. doi: 10.1007/s11414-024-09920-4. Epub 2024 Dec 17. J Behav Health Serv Res. 2025. PMID: 39690392 Free PMC article.
-
Exploring Barriers to Effective COVID-19 Risk Mitigation, Recovery, and Chronic Disease Self-Management: A Qualitative Multilevel Perspective.Patient Relat Outcome Meas. 2024 Sep 18;15:241-253. doi: 10.2147/PROM.S467743. eCollection 2024. Patient Relat Outcome Meas. 2024. PMID: 39310085 Free PMC article.
References
-
- Institute of Medicine (US) Committee on Monitoring Access to Personal Health Care Services; Millman ML, ed. Access to Health Care in America. National Academies Press; 1993. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
