

Early Clinical Outcomes of the Prone Transpsoas Lumbar Interbody Fusion Technique
- PMID: 36690419
- PMCID: PMC10025834
- DOI: 10.14444/8390
Early Clinical Outcomes of the Prone Transpsoas Lumbar Interbody Fusion Technique
Abstract
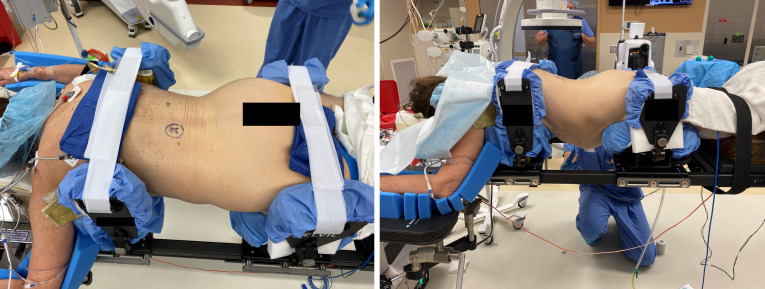
Background: The prone transpsoas (PTP) approach for lateral lumbar interbody fusion (LLIF) is a relatively novel technique. Currently, little is known about its associated complications and early patient-reported outcomes. The aim of this study was to investigate the effect of LLIF performed via the PTP approach on sagittal radiographic parameters, patient-reported outcome measures (PROMs), and rates of complications.
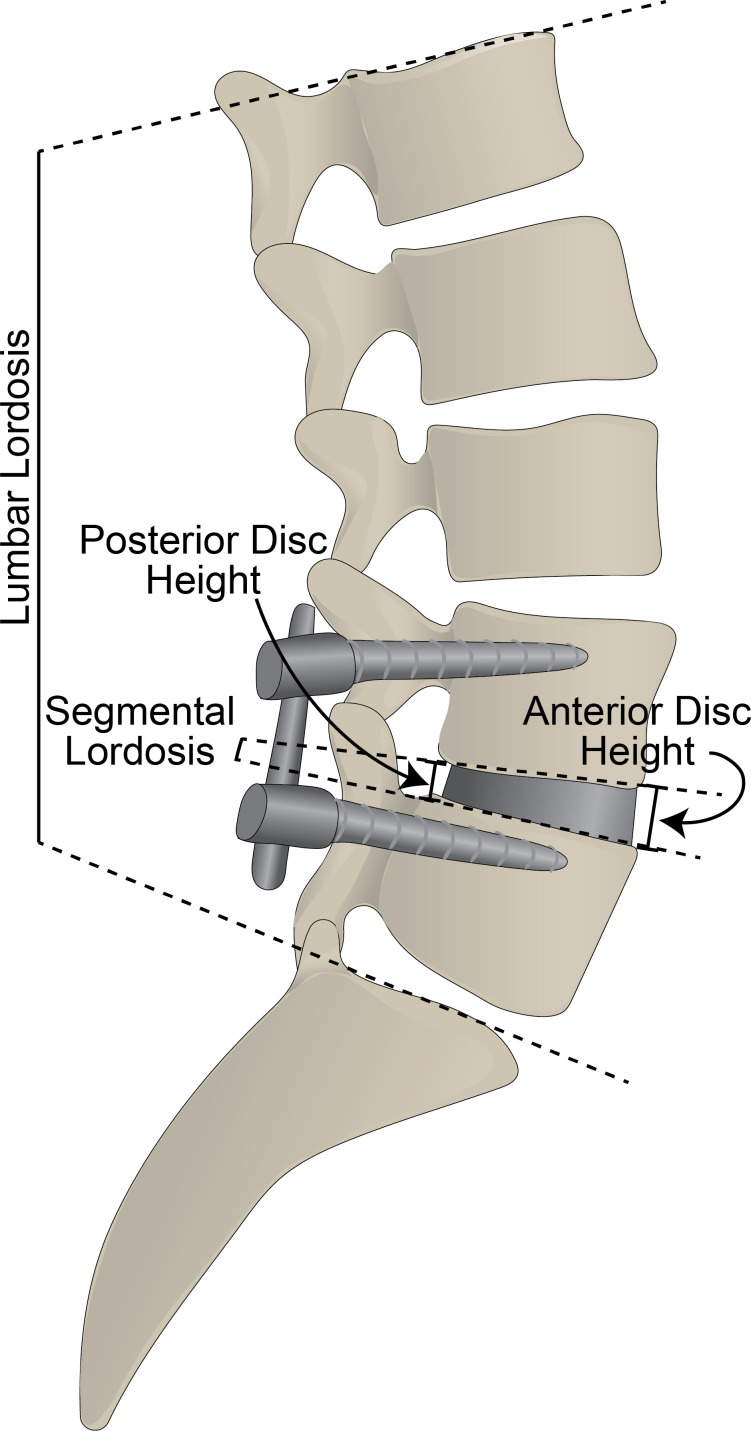
Methods: A retrospective review was performed of 82 consecutive patients who underwent LLIF via a PTP technique. Lumbar lordosis (LL), segmental lordosis (SL), anterior disc height (ADH), and posterior disc height (PDH) were measured on preoperative, initial postoperative, and 3-month postoperative radiographs. PROMs including the Oswestry Disability Index (ODI); the visual analog scale (VAS); and pain portions of the EQ5D, VAS back, and VAS leg ratings were collected at the preoperative and subsequent postoperative visits. Length of hospital stay and postoperative complications related to the procedure were recorded.
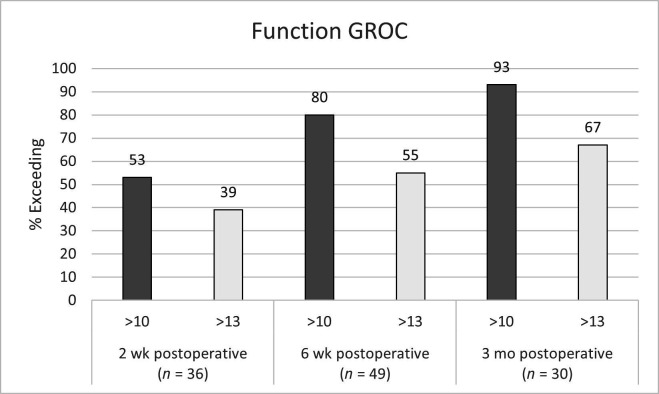
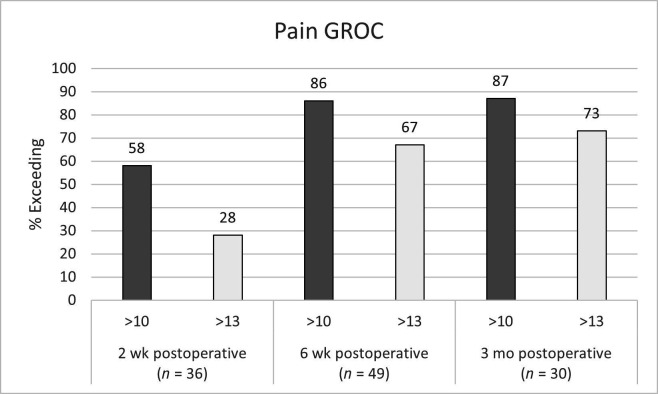
Results: Significant improvements were seen at the initial (4.5° ± 8.6°, P < 0.001) and 3-month (4.4° ± 7.2°, P < 0.001) postoperative periods for LL, as well as SL (6.8° ± 4.8°, P < 0.001; 6.7° ± 4.4°, P < 0.001), ADH (8.0 mm ± 3.6, P < 0.001; 7.4 mm ± 3.6, P < 0.001), and PDH (3.3 mm ± 2.4, P < 0.001; 3.1 mm ± 2.5, P < 0.001). Significant improvements were seen at 3 months postoperatively for ODI (P < 0.001), EQ5D pain (P = 0.016), VAS leg (P < 0.001), and VAS back (P < 0.001). The average length of stay was 2.7 ± 4.5 days. The most common complications were ipsilateral thigh pain/numbness (45.1%), ipsilateral hip flexor weakness (39.0%), and contralateral thigh pain/numbness (14.6%).
Conclusions: While early PROMs and correction of sagittal radiographic parameters show promising results for the PTP approach for LLIF, it is not without risks.
Clinical relevance: PTP interbody fusion is an emerging technique that allows for simultaneous access to the anterior and posterior columns of the lumbar spine. This early case series demonstrates significant improvement in functional outcomes and lumbar lordosis with a safety profile comparable to other well-established techniques.
Keywords: complications; lateral; lumbar; outcomes; prone; psoas.
This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
Conflict of interest statement
Declaration of Conflicting Interests: Hardeep Singh and Isaac Moss are paid consultants for Alphatec.
Figures
Similar articles
-
Clinical Outcomes of Prone Transpsoas Lumbar Interbody Fusion: A 1-Year Follow-Up.Int J Spine Surg. 2024 Sep 12;18(4):400-407. doi: 10.14444/8625. Int J Spine Surg. 2024. PMID: 39084942 Free PMC article.
-
Prone Transpsoas Lateral Interbody Fusion (PTP LIF) with Anterior Docking: Preliminary functional and radiographic outcomes.N Am Spine Soc J. 2023 Sep 28;16:100283. doi: 10.1016/j.xnsj.2023.100283. eCollection 2023 Dec. N Am Spine Soc J. 2023. PMID: 37915968 Free PMC article.
-
Does approach matter? A comparative radiographic analysis of spinopelvic parameters in single-level lumbar fusion.Spine J. 2018 Nov;18(11):1999-2008. doi: 10.1016/j.spinee.2018.03.014. Epub 2018 Apr 6. Spine J. 2018. PMID: 29631061
-
Restoration of lumbar lordosis after minimally invasive transforaminal lumbar interbody fusion: a systematic review.Spine J. 2019 May;19(5):951-958. doi: 10.1016/j.spinee.2018.10.017. Epub 2018 Dec 6. Spine J. 2019. PMID: 30529420
-
Advancing Prone-Transpsoas Spine Surgery: A Narrative Review and Evolution of Indications with Representative Cases.J Clin Med. 2024 Feb 16;13(4):1112. doi: 10.3390/jcm13041112. J Clin Med. 2024. PMID: 38398424 Free PMC article. Review.
Cited by
-
Early Experience with Prone Lateral Interbody Fusion in Deformity Correction: A Single-Institution Experience.J Clin Med. 2024 Apr 15;13(8):2279. doi: 10.3390/jcm13082279. J Clin Med. 2024. PMID: 38673552 Free PMC article.
-
Analyzing the L4-5 Segmental Alignment Change of Two Minimally Invasive Prone-Based Interbody Fusions.Global Spine J. 2025 Apr;15(3):1823-1831. doi: 10.1177/21925682241266165. Epub 2024 Jul 19. Global Spine J. 2025. PMID: 39030673 Free PMC article.
-
Establishment of the prone transpsoas fusion surgery in Australia-a survey and analysis of major complications in early adopters.J Spine Surg. 2025 Mar 24;11(1):15-23. doi: 10.21037/jss-24-128. Epub 2025 Mar 11. J Spine Surg. 2025. PMID: 40242818 Free PMC article.
-
Single-Position Lumbar Fusion Online Videos for Patient Education: Understandability, Reliability, and Quality.J Am Acad Orthop Surg Glob Res Rev. 2025 Aug 19;9(8):e24.00275. doi: 10.5435/JAAOSGlobal-D-24-00275. eCollection 2025 Aug 1. J Am Acad Orthop Surg Glob Res Rev. 2025. PMID: 40828973 Free PMC article.
-
Prone Lateral Transpsoas Approach to the Spine: A Technical Guide for Mastery.Int J Spine Surg. 2025 Feb 24;19(S1):S19-S27. doi: 10.14444/8712. Int J Spine Surg. 2025. PMID: 39819681 Free PMC article.
References
LinkOut - more resources
Full Text Sources