

Natural Course and Prognosis of Primary Spinal Glioblastoma: A Nationwide Study
- PMID: 36690453
- PMCID: PMC10104612
- DOI: 10.1212/WNL.0000000000206834
Natural Course and Prognosis of Primary Spinal Glioblastoma: A Nationwide Study
Abstract
Background and objectives: Primary spinal glioblastoma (PsGBM) is extremely rare. The dramatic neurologic deterioration and unresectability of PsGBM makes it a particularly disabling malignant neoplasm. Because it is a rare and heterogeneous disease, the assessment of prognostic factors remains limited.
Methods: PsGBMs were identified from the French Brain Tumor Database and the Club de Neuro-Oncologie of the Société Française de Neurochirurgie retrospectively. Inclusion criteria were age 18 years or older at diagnosis, spinal location, histopathologic diagnosis of newly glioblastoma according to the 2016 World Health Organization classification, and surgical management between 2004 and 2016. Diagnosis was confirmed by a centralized neuropathologic review. The primary outcome was overall survival (OS). Therapeutic interventions and neurologic outcomes were also collected.
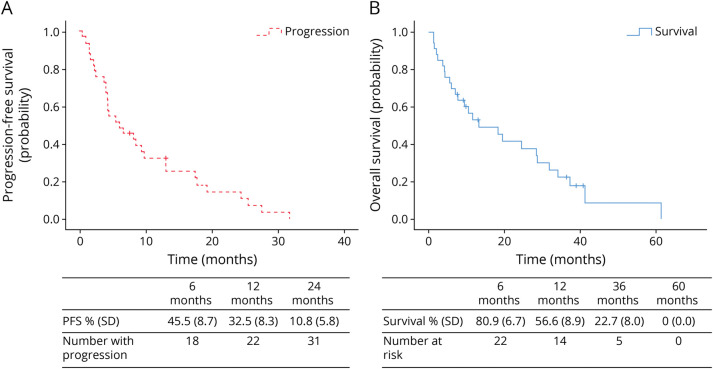
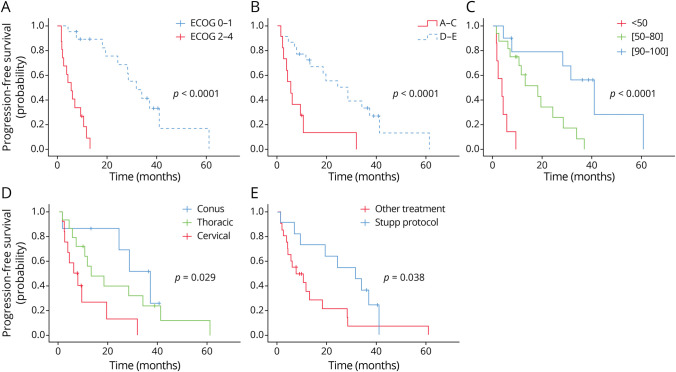
Results: Thirty-three patients with a histopathologically confirmed PsGBM (median age 50.9 years) were included (27 centers). The median OS was 13.1 months (range 2.5-23.7), and the median progression-free survival was 5.9 months (range 1.6-10.2). In multivariable analyses using Cox model, Eastern Cooperative Oncology Group (ECOG) performance status at 0-1 was the only independent predictor of longer OS (hazard ratio [HR] 0.13, 95% CI 0.02-0.801; p = 0.02), whereas a Karnofsky performance status (KPS) score <60 (HR 2.89, 95% CI 1.05-7.92; p = 0.03) and a cervical anatomical location (HR 4.14, 95% CI 1.32-12.98; p = 0.01) were independent predictors of shorter OS. The ambulatory status (Frankel D-E) (HR 0.38, 95% CI 0.07-1.985; p = 0.250) was not an independent prognostic factor, while the concomitant standard radiochemotherapy with temozolomide (Stupp protocol) (HR 0.35, 95% CI 0.118-1.05; p = 0.06) was at the limit of significance.
Discussion: Preoperative ECOG performance status, KPS score, and the location are independent predictors of OS of PsGBMs in adults. Further analyses are required to capture the survival benefit of concomitant standard radiochemotherapy with temozolomide.
© 2023 American Academy of Neurology.
Conflict of interest statement
The authors report no relevant disclosures. Go to
Figures
References
-
- Adams H, Avendaño J, Raza SM, Gokaslan ZL, Jallo GI, Quiñones-Hinojosa A. Prognostic factors and survival in primary malignant astrocytomas of the spinal cord: a population-based analysis from 1973 to 2007. Spine (Phila Pa 1976). 2012;37(12):E727-E735. doi:10.1097/BRS.0b013e31824584c0 - DOI - PMC - PubMed
-
- Ciappetta P, Salvati M, Capoccia G, Artico M, Raco A, Fortuna A. Spinal glioblastomas: report of seven cases and review of the literature. Neurosurgery. 1991;28(2):302-306. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical