

Clinical Subgroups and Factors Associated With Progression in Patients With Inclusion Body Myositis
- PMID: 36690456
- PMCID: PMC10065210
- DOI: 10.1212/WNL.0000000000206777
Clinical Subgroups and Factors Associated With Progression in Patients With Inclusion Body Myositis
Abstract
Background and objectives: Sporadic inclusion body myositis (IBM) is the most common acquired myopathy in individuals older than 50 years. The disorder is slowly progressive, and although many therapies have been investigated, response has generally been poor. Clinical heterogeneity may influence treatment responsiveness; however, data regarding heterogeneity in IBM are limited and often conflicting. We aim to identify clinically distinct subgroups within a large IBM cohort and prognostic factors for disease progression.
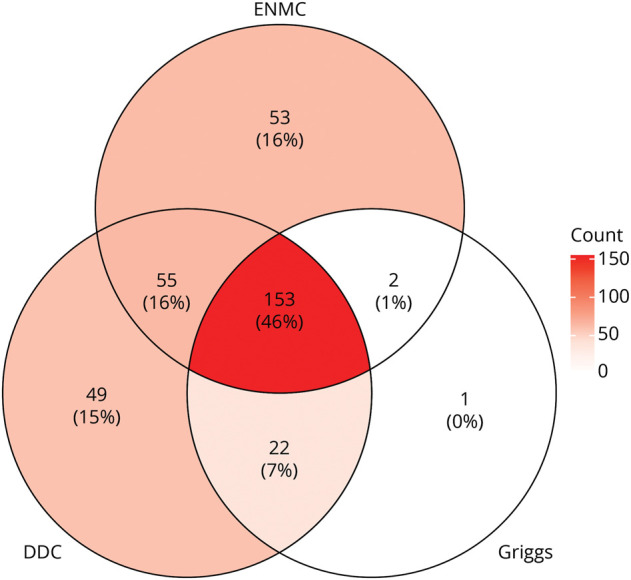
Methods: Clinical, histologic, radiologic, and electrophysiologic data were analyzed for all patients with IBM and other forms of myositis enrolled in a longitudinal cohort from The Johns Hopkins Myositis Center from 2003 to 2018. Patients with IBM were included if they met at least one of the following criteria: Griggs possible, European Neuromuscular Centre 2011 probable, or Lloyd-Greenberg data-derived criteria for IBM. Univariate, multivariate, and graphical analyses were used to identify prognostic factors in patients with IBM. Thus, linear and logistic regressions were used to adjust for potential confounding variables. The evolution of creatine kinase and muscle strength was studied using multilevel linear regression models. Nonmodifiable risk factors (sex, race, disease duration, and age at the onset of first symptoms) were used as adjusting covariates for the regression analyses.
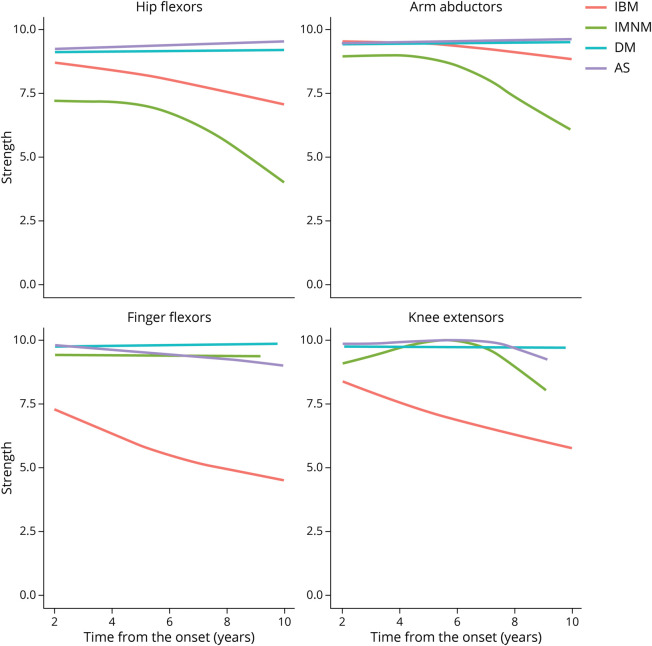
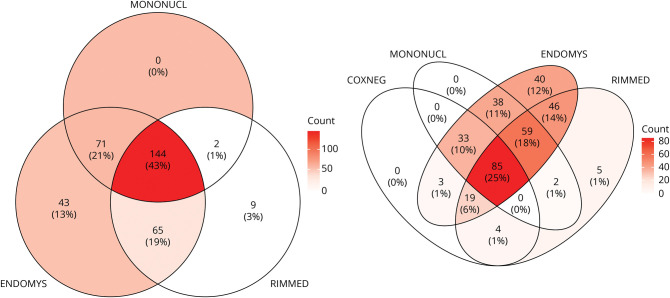
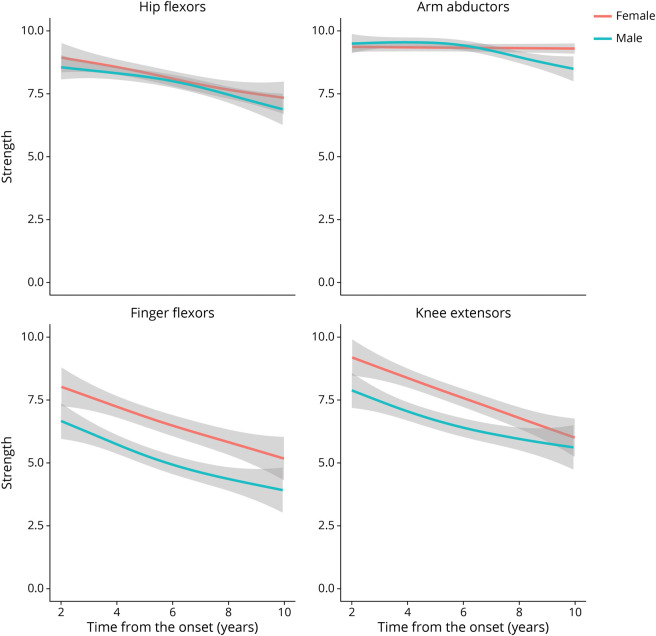
Results: Among the 335 patients meeting the inclusion criteria for IBM, 64% were male with an average age of disease onset of 58.7 years and delay to diagnosis of 5.2 years. Initial misdiagnosis (52%) and immunosuppressant treatment (42%) were common. Less than half (43%) of muscle biopsies demonstrated all 3 pathologic hallmarks: endomysial inflammation, mononuclear cell invasion, and rimmed vacuoles. Black patients had significantly weaker arm abductors, hip flexors, and knee flexors compared with non-Black patients. Female patients had stronger finger flexors and knee extensors compared with their male counterparts. Younger age (<50 years) at onset was not associated with increased weakness.
Discussion: Our study demonstrates that female and Black patients have distinct clinical phenotypes and trajectories within the overarching IBM clinical phenotype. These subgroups may have different responses to therapies, which may influence the design of future clinical trials in IBM.
© 2023 American Academy of Neurology.
Conflict of interest statement
E.H. Michelle reports funding from The Sandra and Malcolm Berman Brain & Spine Institute. I. Pinal-Fernandez received support from The Intramural Research Program of the National Institute of Arthritis and Musculoskeletal and Skin Diseases, NIH. M. Casal-Dominguez received support from The Intramural Research Program of the National Institute of Arthritis and Musculoskeletal and Skin Diseases, NIH. J. Albayda was supported by contributions from The Peter and Carmen Lucia Buck Foundation and The Huayi and Siuling Zhang Discovery Fund. J.J. Paik was supported by funding from The National Institute of Arthritis and Musculoskeletal and Skin Diseases of the NIH under award number K23AR073927 and contributions from The Peter and Carmen Lucia Buck Foundation and The Huayi and Siuling Zhang Discovery Fund. E. Tiniakou was supported by contributions from The Peter and Carmen Lucia Buck Foundation and The Huayi and Siuling Zhang Discovery Fund. B. Adler was supported by contributions from The Peter and Carmen Lucia Buck Foundation and The Huayi and Siuling Zhang Discovery Fund. C.A. Mecoli was supported by contributions from The Peter and Carmen Lucia Buck Foundation and The Huayi and Siuling Zhang Discovery Fund. S.K. Danoff was supported by contributions from The Peter and Carmen Lucia Buck Foundation and The Huayi and Siuling Zhang Discovery Fund. L. Christopher-Stine was supported by contributions from The Peter and Carmen Lucia Buck Foundation and The Huayi and Siuling Zhang Discovery Fund. A.L. Mammen was supported by The Intramural Research Program of the National Institute of Arthritis and Musculoskeletal and Skin Diseases, NIH. T.E. Lloyd was supported by R01 AR076390 from NIAMS/NIH and MDA630399 from the Muscular Dystrophy Association and by contributions from The Peter and Carmen Lucia Buck Foundation and The Huayi and Siuling Zhang Discovery Fund. Go to
Figures
Comment in
-
Reader Response: Clinical Subgroups and Factors Associated With Progression in Patients With Inclusion Body Myositis.Neurology. 2023 Sep 12;101(11):499-500. doi: 10.1212/WNL.0000000000207783. Neurology. 2023. PMID: 37696674 Free PMC article. No abstract available.
-
Author Response: Clinical Subgroups and Factors Associated With Progression in Patients With Inclusion Body Myositis.Neurology. 2023 Sep 12;101(11):500. doi: 10.1212/WNL.0000000000207784. Neurology. 2023. PMID: 37696675 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous