

Preoperative hemoglobin and perioperative blood transfusion in major head and neck surgery: a systematic review and meta-analysis
- PMID: 36691071
- PMCID: PMC9872343
- DOI: 10.1186/s40463-022-00588-4
Preoperative hemoglobin and perioperative blood transfusion in major head and neck surgery: a systematic review and meta-analysis
Abstract
Background: There is a growing concern with inappropriate, excessive perioperative blood transfusions. Understanding the influence of low preoperative hemoglobin (Hgb) on perioperative blood transfusion (PBT) in head and neck cancer (HNC) surgery with free flap reconstruction may help guide clinical practice to reduce inappropriate treatment among these patients. The objective is to synthesize evidence regarding the association between preoperative Hgb and PBT among major HNC free flap surgeries.
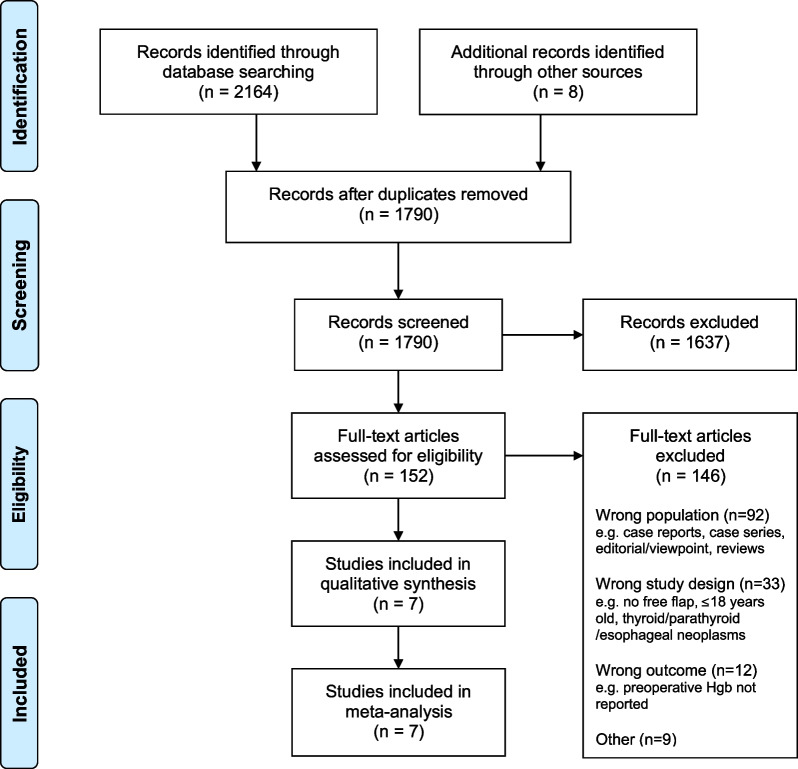
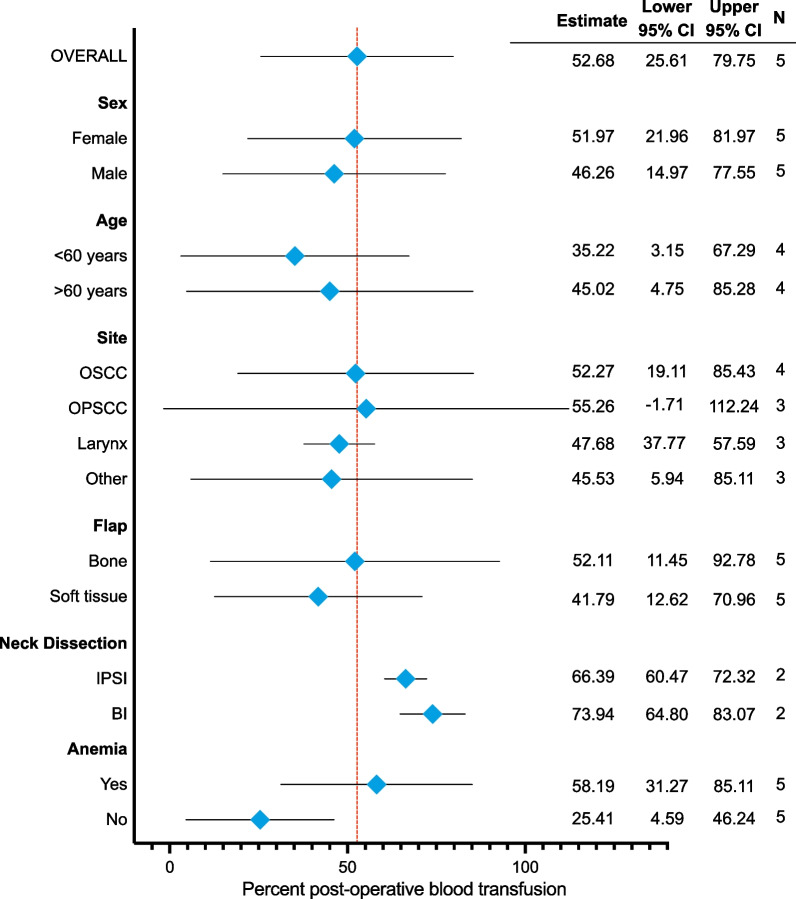
Methods: Terms and synonyms for HNC surgical procedures, Hgb and PBT were used to search MEDLINE, Embase, CINAHL, Cochrane Central Register of Controlled Trials and Cochrane Database of Reviews from inception to February 2020. Reference lists of included full texts and studies reporting the preoperative Hgb, anemia or hematocrit (exposure) and the PBT (outcome) in major HNC surgery with free flap reconstruction were eligible. Studies examining esophageal, thyroid and parathyroid neoplasms were excluded; as were case reports, case series (n < 20), editorials, reviews, perspectives, viewpoints and responses. Two independent, blinded reviewers screened titles, abstracts and full texts in duplicate. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses was followed. A random-effects model was used to pool reported data. The primary outcome was the proportion of patients who had a PBT. Subgroup analysis examined sources of heterogeneity for perioperative predictors of PBT (age, sex, flap type, flap site and preoperative Hgb). We also examined mean preoperative Hgb in the PBT and no PBT groups.
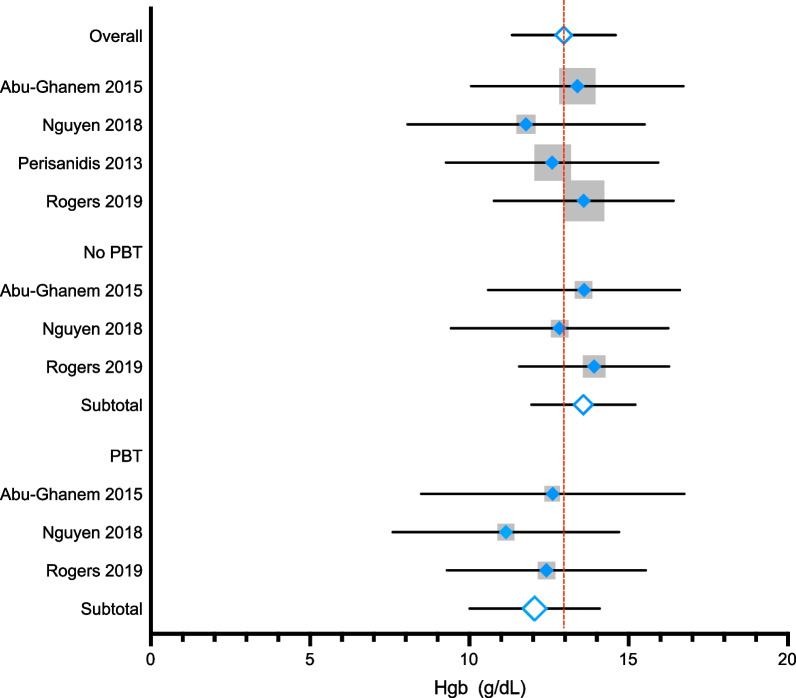
Results: Patients with low preoperative Hgb were transfused more than those with normal Hgb (47.62%, 95% CI = 41.19-54.06, I2 = 0.00% and 13.92%, 95% CI = 10.19-17.65, I2 = 20.69%, respectively). None of the predictor variables explained PBT. The overall pooled mean preoperative Hgb was 12.96 g/dL (95% CI = 11.33-14.59, I2 = 0.00%) and was 13.58 g/dL (95% CI = 11.95-15.21, I2 = 0.00%) in the no PBT group and 12.05 g/dL (95% CI = 10.01 to 14.09, I2 = 0.00%) in the PBT group.
Conclusions: The heterogeneity between studies, especially around the trigger for PBT, highlights the need for additional research to guide clinical practice of preoperative Hgb related to PBT to enhance patient outcomes and improve healthcare stewardship.
Keywords: Blood transfusion; ENT; Ears nose throat; Free flap reconstruction; Free tissue transfer; Head and neck cancer; Head and neck carcinoma; Head and neck neoplasms; Head and neck surgery; Meta-analysis; Otolaryngology; Otorhinolaryngology; Preoperative anemia; Systematic review.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Preoperative anemia and perioperative blood transfusion in head and neck squamous cell carcinoma.PLoS One. 2018 Oct 22;13(10):e0205712. doi: 10.1371/journal.pone.0205712. eCollection 2018. PLoS One. 2018. PMID: 30347001 Free PMC article.
-
Predictive factors for perioperative blood transfusion in neck dissection.Laryngoscope. 2016 Apr;126(4):851-7. doi: 10.1002/lary.25639. Epub 2015 Sep 15. Laryngoscope. 2016. PMID: 26371773
-
A model for predicting transfusion requirements in head and neck surgery.Laryngoscope. 1995 Aug;105(8 Pt 2 Suppl 73):1-17. doi: 10.1288/00005537-199508001-00001. Laryngoscope. 1995. PMID: 7630307 Review.
-
What Should Define Preoperative Anemia in Primary THA?Clin Orthop Relat Res. 2017 Nov;475(11):2683-2691. doi: 10.1007/s11999-017-5469-4. Epub 2017 Aug 7. Clin Orthop Relat Res. 2017. PMID: 28786087 Free PMC article.
-
Role of preoperative intravenous iron therapy to correct anemia before major surgery: a systematic review and meta-analysis.Syst Rev. 2021 Jan 23;10(1):36. doi: 10.1186/s13643-021-01579-8. Syst Rev. 2021. PMID: 33485392 Free PMC article.
Cited by
-
Opioid-Free Anaesthesia Reduces Complications in Head and Neck Microvascular Free-Flap Reconstruction.J Clin Med. 2023 Oct 10;12(20):6445. doi: 10.3390/jcm12206445. J Clin Med. 2023. PMID: 37892584 Free PMC article.
-
The Effect of Preoperative Anemia on Blood Transfusion Outcomes in Major Head and Neck Cancer Surgery.Cancers (Basel). 2025 Jun 25;17(13):2136. doi: 10.3390/cancers17132136. Cancers (Basel). 2025. PMID: 40647435 Free PMC article.
-
Preoperative iron supplementation in non-anemic patients undergoing major surgery: a systematic review and meta-analysis.Braz J Anesthesiol. 2025 May-Jun;75(3):844618. doi: 10.1016/j.bjane.2025.844618. Epub 2025 Apr 4. Braz J Anesthesiol. 2025. PMID: 40189047 Free PMC article.
-
An Investigation Into the Risk Factors for Transfusion Need After Neck of Femur Fracture Surgery.Cureus. 2024 Aug 24;16(8):e67673. doi: 10.7759/cureus.67673. eCollection 2024 Aug. Cureus. 2024. PMID: 39314585 Free PMC article.
References
-
- Kim L, King T, Agulnik M. Head and neck cancer: changing epidemiology and public health implications. Oncology. 2010;24(10):915. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
