

Contrast enhanced mammography: focus on frequently encountered benign and malignant diagnoses
- PMID: 36691077
- PMCID: PMC9872331
- DOI: 10.1186/s40644-023-00526-1
Contrast enhanced mammography: focus on frequently encountered benign and malignant diagnoses
Abstract
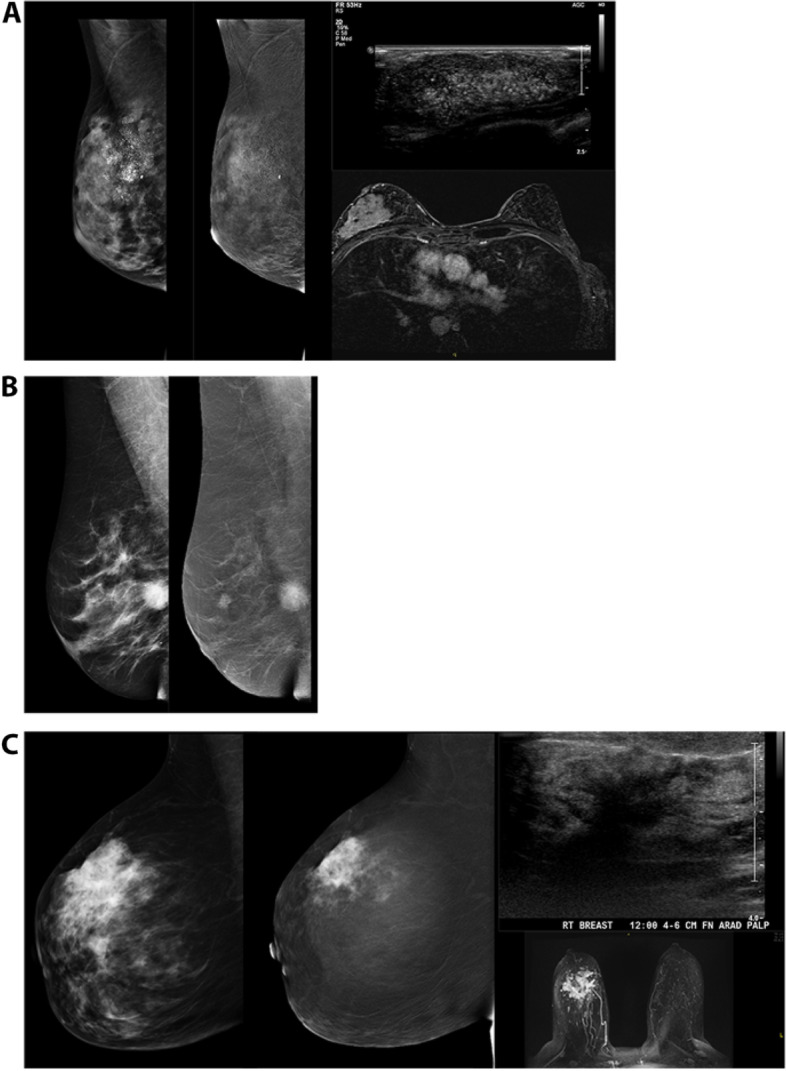
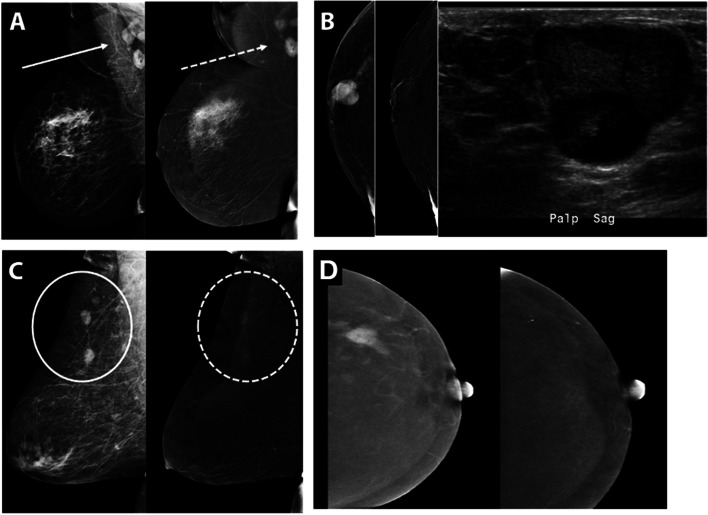
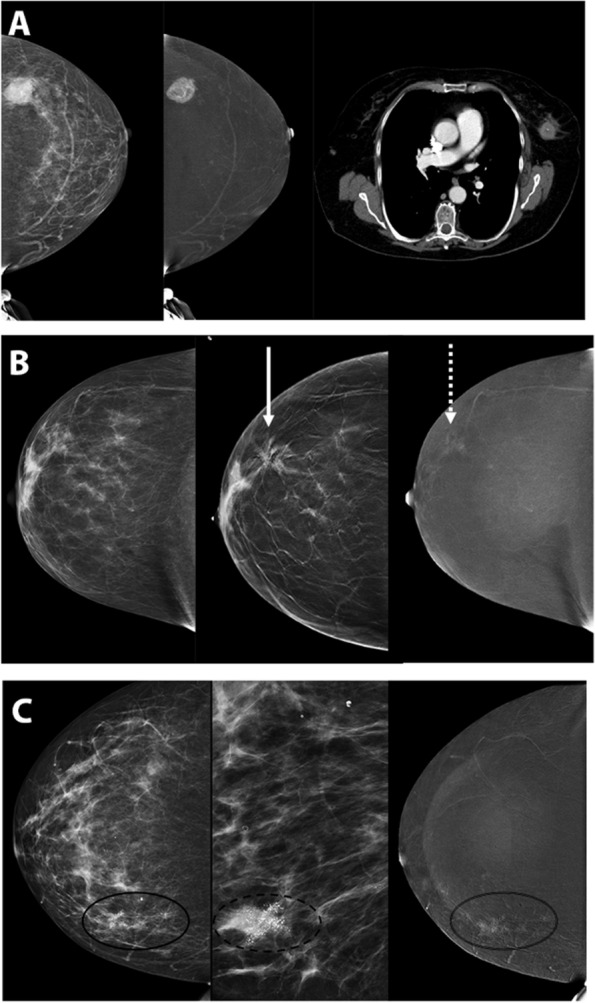
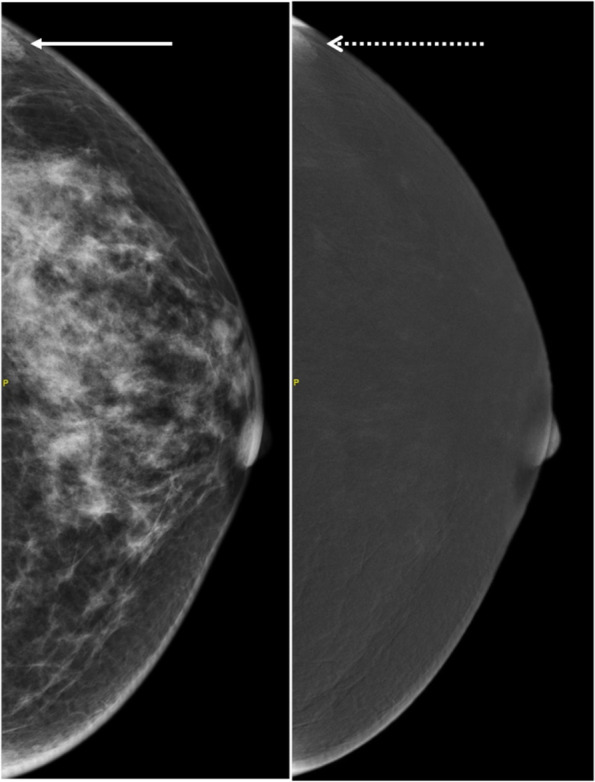
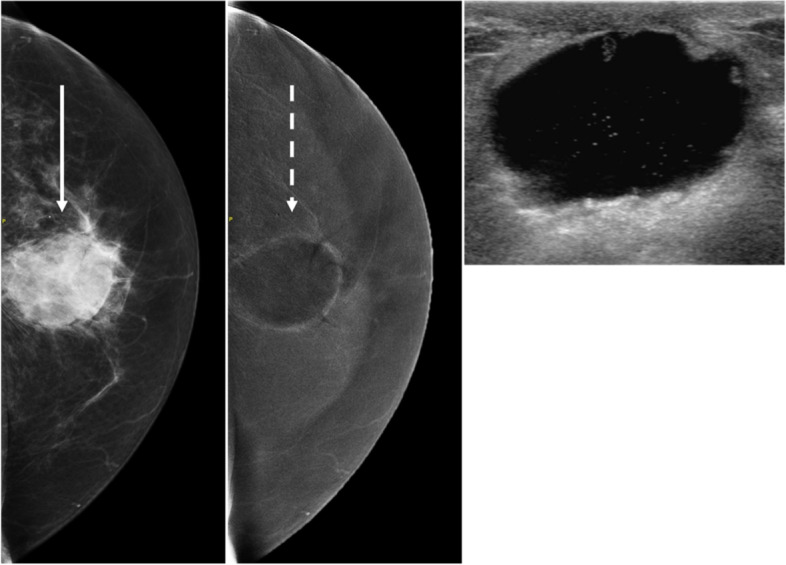
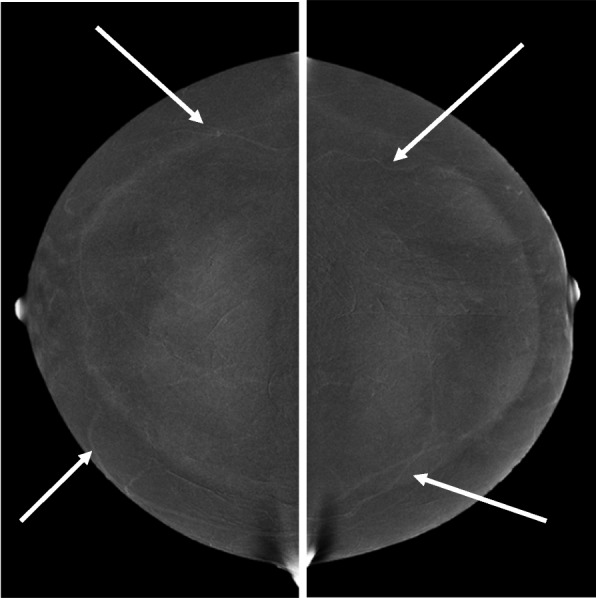
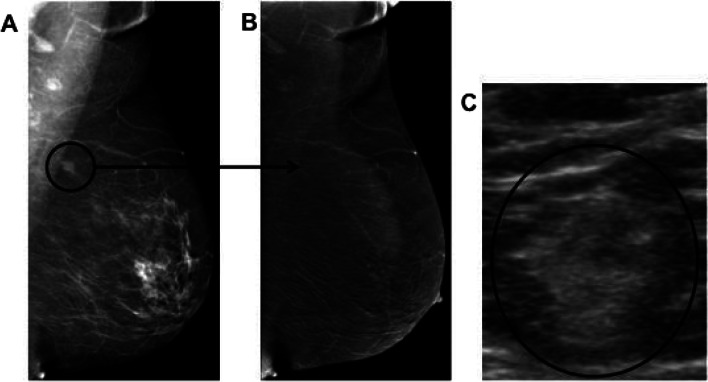
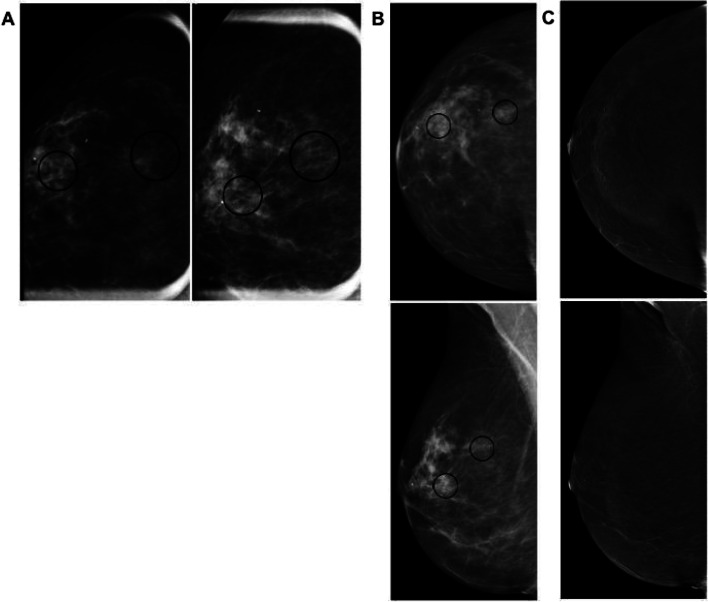
Contrast-enhanced mammography (CEM) is becoming a widely adopted modality in breast imaging over the past few decades and exponentially so over the last few years, with strong evidence of high diagnostic performance in cancer detection. Evidence is also growing indicating comparative performance of CEM to MRI in sensitivity with fewer false positive rates. As application of CEM ranges from potential use in screening dense breast populations to staging of known breast malignancy, increased familiarity with the modality and its implementation, and disease processes encountered becomes of great clinical significance. This review emphasizes expected normal findings on CEM followed by a focus on examples of the commonly encountered benign and malignant pathologies on CEM.
Keywords: Contrast mammography; Contrast-enhanced mammography; Mammography.
© 2023. The Author(s).
Conflict of interest statement
There are no potential competing interests for the authors.
The Authors declare no Competing Financial or Non-Financial Interests.
Figures
Similar articles
-
Comparison of Performance in Diagnosis and Characterization of Breast Lesions: Contrast-Enhanced Mammography Versus Breast Magnetic Resonance Imaging.Clin Breast Cancer. 2024 Aug;24(6):481-493. doi: 10.1016/j.clbc.2024.04.007. Epub 2024 Apr 15. Clin Breast Cancer. 2024. PMID: 38777678
-
Patient preferences regarding use of contrast-enhanced imaging for breast cancer screening.Acad Radiol. 2022 Jan;29 Suppl 1:S229-S238. doi: 10.1016/j.acra.2021.03.003. Epub 2021 Apr 9. Acad Radiol. 2022. PMID: 33846061
-
Contrast-enhanced Mammography versus Contrast-enhanced Breast MRI: A Systematic Review and Meta-Analysis.Radiology. 2022 Oct;305(1):94-103. doi: 10.1148/radiol.212530. Epub 2022 Jun 7. Radiology. 2022. PMID: 36154284
-
The PROCEM study protocol: Added value of preoperative contrast-enhanced mammography in staging of malignant breast lesions - a prospective randomized multicenter study.BMC Cancer. 2021 Oct 18;21(1):1115. doi: 10.1186/s12885-021-08832-2. BMC Cancer. 2021. PMID: 34663236 Free PMC article.
-
Preoperative evaluation of breast cancer: Contrast-enhanced mammography versus contrast-enhanced magnetic resonance imaging: A systematic review and meta-analysis.Breast Dis. 2022;41(1):303-315. doi: 10.3233/BD-210034. Breast Dis. 2022. PMID: 35754256
Cited by
-
Diagnostic dilemma of lobular carcinoma: a mini-review of imaging modalities and the role of artificial intelligence and radiomics.Front Oncol. 2025 Mar 27;15:1515037. doi: 10.3389/fonc.2025.1515037. eCollection 2025. Front Oncol. 2025. PMID: 40212677 Free PMC article. Review.
-
Contrast-Enhanced Mammography in Breast Lesion Assessment: Accuracy and Surgical Impact.Tomography. 2025 Aug 20;11(8):93. doi: 10.3390/tomography11080093. Tomography. 2025. PMID: 40863884 Free PMC article.
-
Diagnostic Efficacy of Five Different Imaging Modalities in the Assessment of Women Recalled at Breast Screening-A Systematic Review and Meta-Analysis.Cancers (Basel). 2024 Oct 17;16(20):3505. doi: 10.3390/cancers16203505. Cancers (Basel). 2024. PMID: 39456600 Free PMC article. Review.
-
Contrast-enhanced mammography-based interpretable machine learning model for the prediction of the molecular subtype breast cancers.BMC Med Imaging. 2025 Jul 1;25(1):255. doi: 10.1186/s12880-025-01765-3. BMC Med Imaging. 2025. PMID: 40596940 Free PMC article.
-
Role of contrast-enhanced mammogram as an adjunct to tomosynthesis in evaluation of circumscribed breast lesions.Br J Radiol. 2024 Oct 1;97(1162):1696-1705. doi: 10.1093/bjr/tqae130. Br J Radiol. 2024. PMID: 39024041 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
