

COVID-19 bacteremic co-infection is a major risk factor for mortality, ICU admission, and mechanical ventilation
- PMID: 36691080
- PMCID: PMC9868503
- DOI: 10.1186/s13054-023-04312-0
COVID-19 bacteremic co-infection is a major risk factor for mortality, ICU admission, and mechanical ventilation
Abstract
Background: Recent single-center reports have suggested that community-acquired bacteremic co-infection in the context of Coronavirus disease 2019 (COVID-19) may be an important driver of mortality; however, these reports have not been validated with a multicenter, demographically diverse, cohort study with data spanning the pandemic.
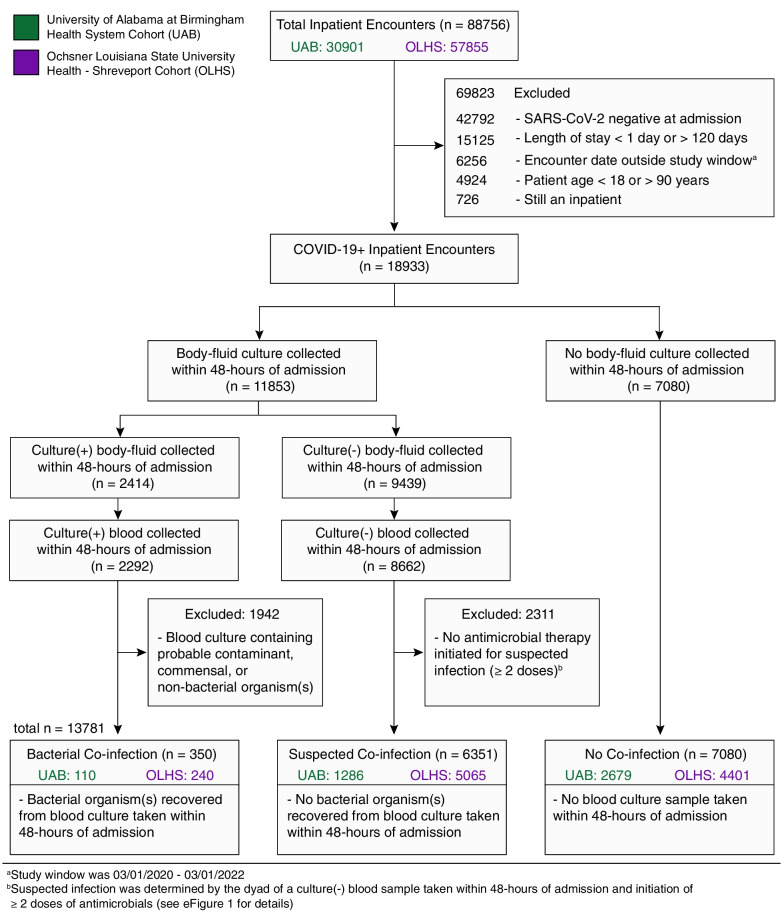
Methods: In this multicenter, retrospective cohort study, inpatient encounters were assessed for COVID-19 with community-acquired bacteremic co-infection using 48-h post-admission blood cultures and grouped by: (1) confirmed co-infection [recovery of bacterial pathogen], (2) suspected co-infection [negative culture with ≥ 2 antimicrobials administered], and (3) no evidence of co-infection [no culture]. The primary outcomes were in-hospital mortality, ICU admission, and mechanical ventilation. COVID-19 bacterial co-infection risk factors and impact on primary outcomes were determined using multivariate logistic regressions and expressed as adjusted odds ratios with 95% confidence intervals (Cohort, OR 95% CI, Wald test p value).
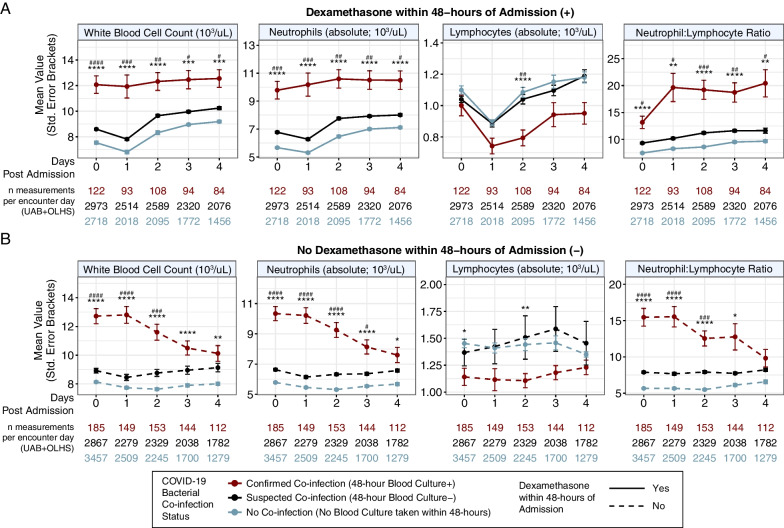
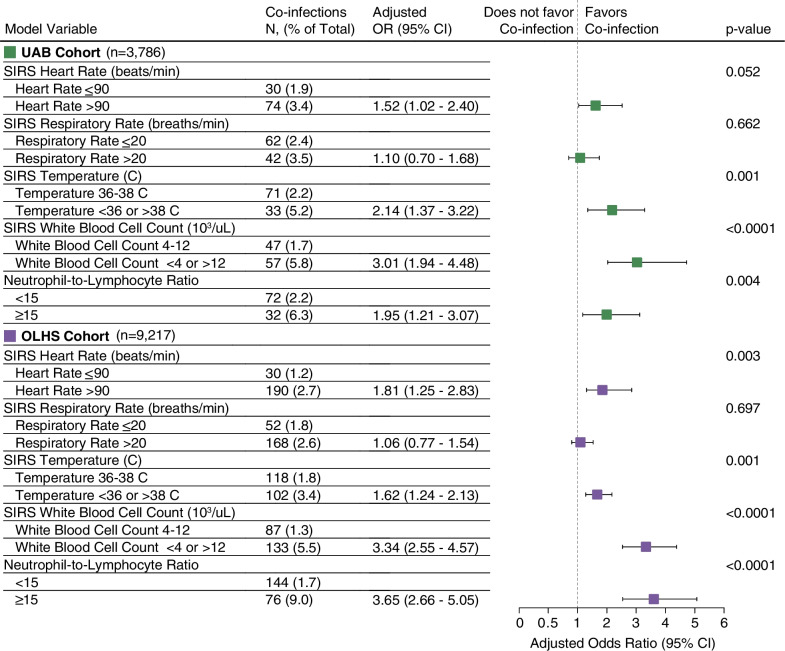
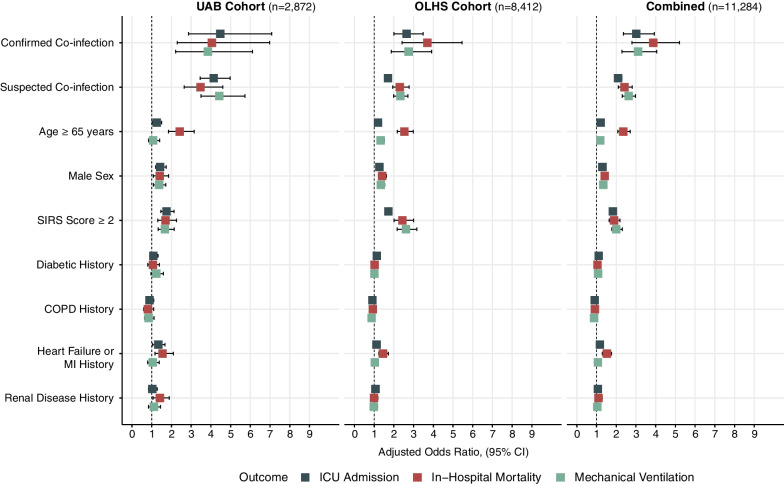
Results: The studied cohorts included 13,781 COVID-19 inpatient encounters from 2020 to 2022 in the University of Alabama at Birmingham (UAB, n = 4075) and Ochsner Louisiana State University Health-Shreveport (OLHS, n = 9706) cohorts with confirmed (2.5%), suspected (46%), or no community-acquired bacterial co-infection (51.5%) and a comparison cohort consisting of 99,170 inpatient encounters from 2010 to 2019 (UAB pre-COVID-19 pandemic cohort). Significantly increased likelihood of COVID-19 bacterial co-infection was observed in patients with elevated ≥ 15 neutrophil-to-lymphocyte ratio (UAB: 1.95 [1.21-3.07]; OLHS: 3.65 [2.66-5.05], p < 0.001 for both) within 48-h of hospital admission. Bacterial co-infection was found to confer the greatest increased risk for in-hospital mortality (UAB: 3.07 [2.42-5.46]; OLHS: 4.05 [2.29-6.97], p < 0.001 for both), ICU admission (UAB: 4.47 [2.87-7.09], OLHS: 2.65 [2.00-3.48], p < 0.001 for both), and mechanical ventilation (UAB: 3.84 [2.21-6.12]; OLHS: 2.75 [1.87-3.92], p < 0.001 for both) across both cohorts, as compared to other risk factors for severe disease. Observed mortality in COVID-19 bacterial co-infection (24%) dramatically exceeds the mortality rate associated with community-acquired bacteremia in pre-COVID-19 pandemic inpatients (5.9%) and was consistent across alpha, delta, and omicron SARS-CoV-2 variants.
Conclusions: Elevated neutrophil-to-lymphocyte ratio is a prognostic indicator of COVID-19 bacterial co-infection within 48-h of admission. Community-acquired bacterial co-infection, as defined by blood culture-positive results, confers greater increased risk of in-hospital mortality, ICU admission, and mechanical ventilation than previously described risk factors (advanced age, select comorbidities, male sex) for COVID-19 mortality, and is independent of SARS-CoV-2 variant.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Comparison of clinical outcomes in critically ill COVID-19 patients on mechanical ventilation with nosocomial pneumonia between Alpha and Omicron variants.Ther Adv Respir Dis. 2023 Jan-Dec;17:17534666231213642. doi: 10.1177/17534666231213642. Ther Adv Respir Dis. 2023. PMID: 38018405 Free PMC article.
-
Hospital Outcomes of Community-Acquired SARS-CoV-2 Omicron Variant Infection Compared With Influenza Infection in Switzerland.JAMA Netw Open. 2023 Feb 1;6(2):e2255599. doi: 10.1001/jamanetworkopen.2022.55599. JAMA Netw Open. 2023. PMID: 36790812 Free PMC article.
-
Risk Factors Associated With Mortality Among Patients With COVID-19 in Intensive Care Units in Lombardy, Italy.JAMA Intern Med. 2020 Oct 1;180(10):1345-1355. doi: 10.1001/jamainternmed.2020.3539. JAMA Intern Med. 2020. PMID: 32667669 Free PMC article.
-
Global Impact of Coronavirus Disease 2019 Infection Requiring Admission to the ICU: A Systematic Review and Meta-analysis.Chest. 2021 Feb;159(2):524-536. doi: 10.1016/j.chest.2020.10.014. Epub 2020 Oct 15. Chest. 2021. PMID: 33069725 Free PMC article.
-
Obesity in patients with COVID-19: a systematic review and meta-analysis.Metabolism. 2020 Dec;113:154378. doi: 10.1016/j.metabol.2020.154378. Epub 2020 Sep 28. Metabolism. 2020. PMID: 33002478 Free PMC article.
Cited by
-
Mortality in hospitalized SARS-CoV-2 patients with contemporaneous bacterial and fungal infections.Antimicrob Steward Healthc Epidemiol. 2024 Sep 23;4(1):e142. doi: 10.1017/ash.2024.424. eCollection 2024. Antimicrob Steward Healthc Epidemiol. 2024. PMID: 39346658 Free PMC article.
-
Implications of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infected Hospitalised Patients with Co-Infections and Clinical Outcomes.Microorganisms. 2023 Jul 28;11(8):1921. doi: 10.3390/microorganisms11081921. Microorganisms. 2023. PMID: 37630481 Free PMC article.
-
The Real Impact of Age on Mortality in Critically Ill COVID-19 Patients.J Pers Med. 2023 May 29;13(6):908. doi: 10.3390/jpm13060908. J Pers Med. 2023. PMID: 37373897 Free PMC article.
-
Genetically predicted blood metabolites mediate the association between circulating immune cells and severe COVID-19: A Mendelian randomization study.Medicine (Baltimore). 2024 Nov 15;103(46):e40509. doi: 10.1097/MD.0000000000040509. Medicine (Baltimore). 2024. PMID: 39560514 Free PMC article.
-
Dual threat: Susceptibility mechanisms and treatment strategies for COVID-19 and bacterial co-infections.Comput Struct Biotechnol J. 2025 May 22;27:2107-2122. doi: 10.1016/j.csbj.2025.05.033. eCollection 2025. Comput Struct Biotechnol J. 2025. PMID: 40502935 Free PMC article. Review.
References
-
- World Health Organization. Weekly epidemiological update on COVID-19 - 3 August 2022. Emergency Situational Updates, 2022; 103. http://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation...
-
- Russell CD, Fairfield CJ, Drake TM, et al. Co-infections, secondary infections, and antimicrobial use in patients hospitalised with COVID-19 during the first pandemic wave from the ISARIC WHO CCP-UK study: a multicentre, prospective cohort study. Lancet Microbe. 2021;2:e354–e365. doi: 10.1016/S2666-5247(21)00090-2. - DOI - PMC - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
