

Global, regional and national trends in statin utilisation in high-income and low/middle-income countries, 2015-2020
- PMID: 36691204
- PMCID: PMC9462115
- DOI: 10.1136/bmjopen-2022-061350
Global, regional and national trends in statin utilisation in high-income and low/middle-income countries, 2015-2020
Abstract
Objective: Prior studies have reported inequitable global access to essential medicines for cardiovascular disease (CVD) prevention, especially statins. Here we examine recent trends and disparities in statin utilisation at the income group, regional and country levels.
Design: Ecological study. Pharmaceutical sales data were used to examine statin utilisation in high-income counties (HICs) and low/middle-income countries (LMICs) from 2015 to 2020. Population estimates were obtained from the Global Burden of Disease. Fixed-effects panel regression analysis was used to examine associations between statin utilisation and country-level factors.
Setting: Global, including 41 HICs and 50 LMICs.
Participants: Population older than 40 years of age.
Primary and secondary outcome measures: Statin utilisation was measured using defined daily doses (DDDs) per 1000 population ≥40 years per day (TPD).
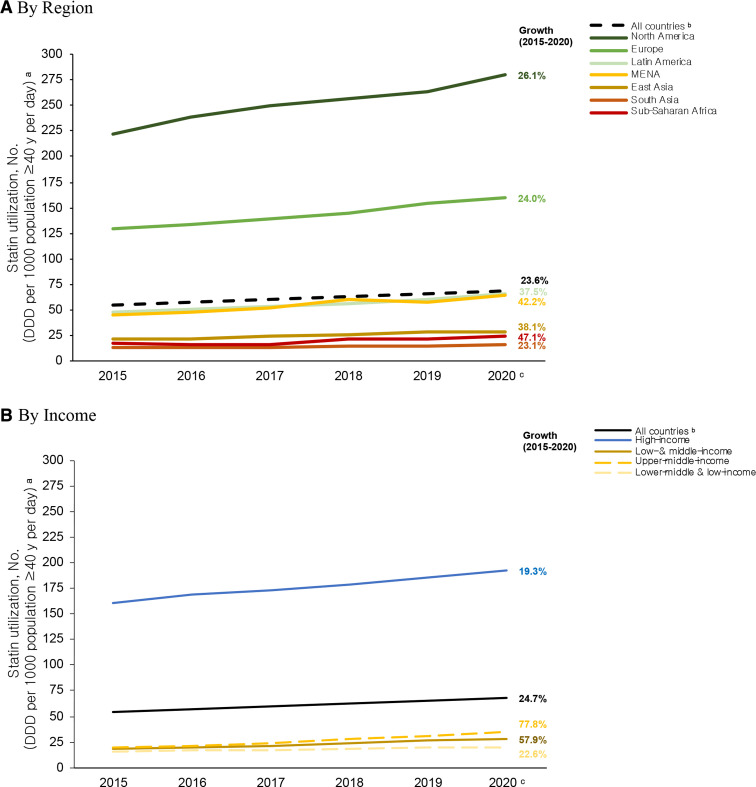
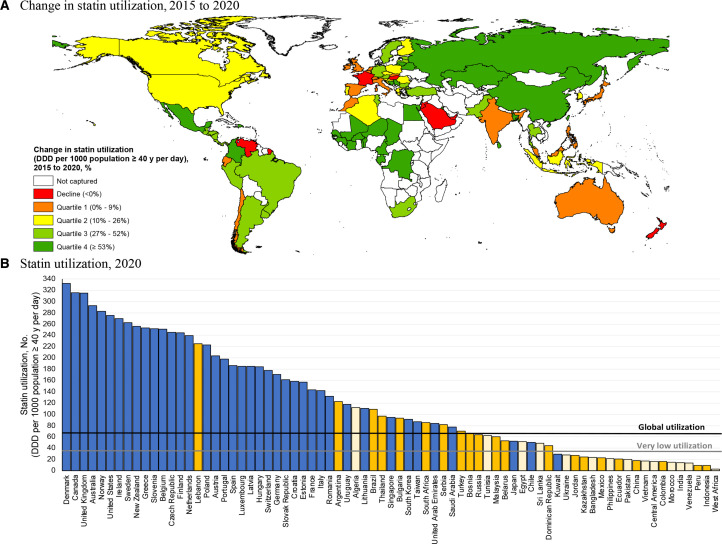
Results: Globally, statin utilisation increased 24.7% from 54.7 DDDs/TPD in 2015 to 68.3 DDDs/TPD in 2020. However, regional and income group disparities persisted during this period. In 2020, statin utilisation was more than six times higher in HICs than LMICs (192.4 vs 28.4 DDDs/TPD, p<0.01). Substantial disparities were also observed between LMICs, ranging from 3.1 DDDs/TPD in West African nations to 225.0 DDDs/TPD in Lebanon in 2020. While statin utilisation increased in most LMICs between 2015 and 2020, several experienced declines in utilisation, most notably Venezuela (-85.1%, from 92.3 to 14.0 DDDs/TPD). In LMICs, every $100 increase in per capita health spending was associated with a 17% increase in statin utilisation, while every 10% increase in out-of-pocket health spending was associated with a 11% decline (both p<0.05).
Conclusions: Despite global increases in statin utilisation, there are substantial regional and country-level disparities between HICs and LMICs. To address global CVD disparities, policymakers should promote increased and equitable access to statins in LMICs.
Keywords: Health policy; Ischaemic heart disease; PUBLIC HEALTH.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JSG currently reports employment with Flatiron Health, which is an independent subsidiary of the Roche Group.
Figures
References
-
- World Health Organization . Prevention of cardiovascular disease: guidelines for assessment and management of cardiovascular risk, 2007. Available: https://www.who.int/cardiovascular_diseases/guidelines [Accessed 24 Oct 2021].
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical