

Investigating Racial and Socioeconomic Characteristics in Pediatric Sepsis Using Electronic Health Data
- PMID: 36691761
- PMCID: PMC10680400
- DOI: 10.1542/hpeds.2022-006752
Investigating Racial and Socioeconomic Characteristics in Pediatric Sepsis Using Electronic Health Data
Abstract
Background and objectives: Racial/ethnic and socioeconomic disparities are reported in sepsis, with increased mortality for minority and low socioeconomic status groups; however, these studies rely on billing codes that are imprecise in identifying sepsis. Using a previously validated algorithm to detect pediatric sepsis using electronic clinical data, we hypothesized that racial/ethnic and socioeconomic status disparities would be evident in this group.
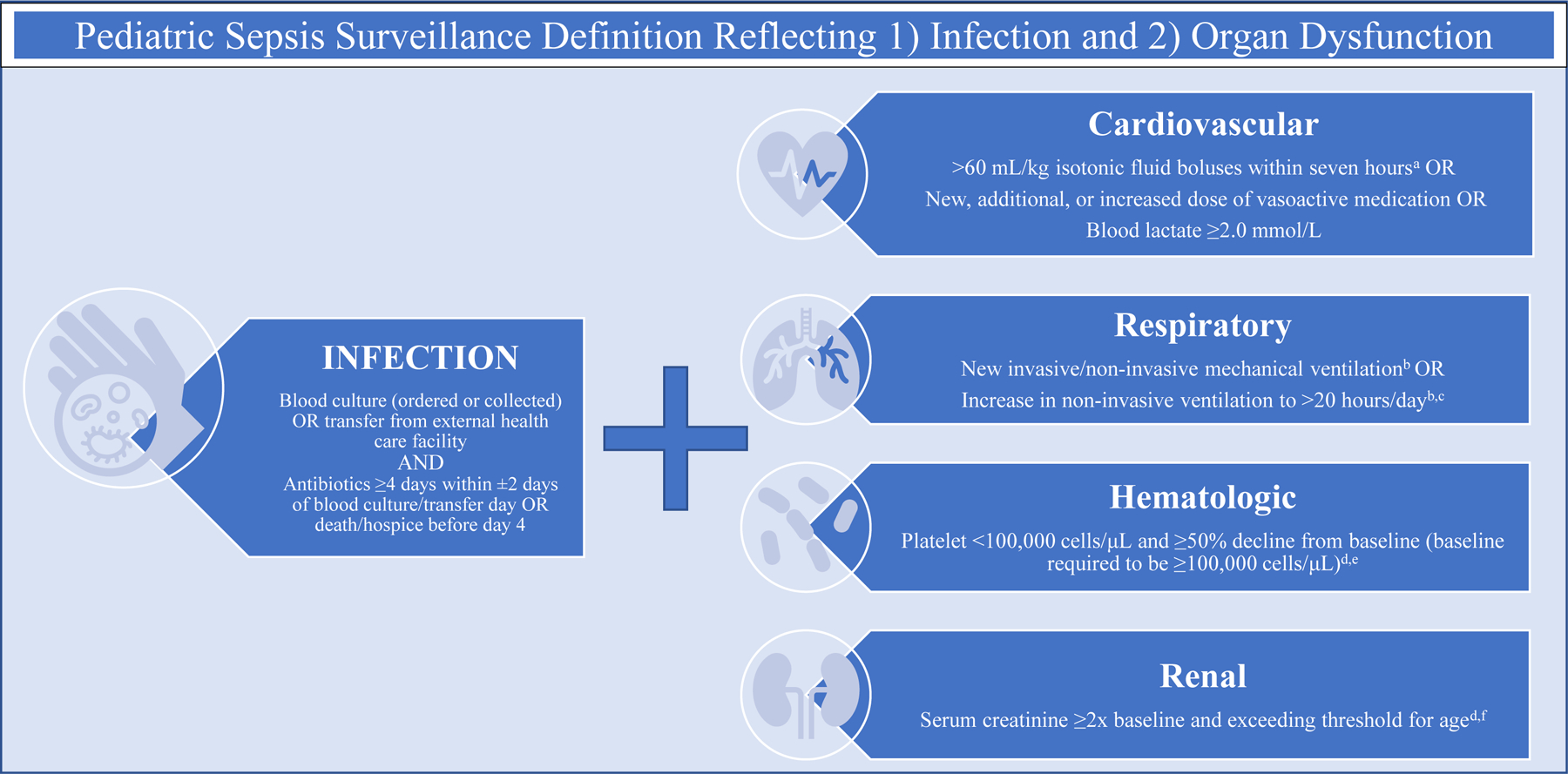
Methods: We performed a retrospective study from a large, quaternary academic center, including sepsis episodes from January 20, 2011, to May 20, 2021, identified by an algorithm indicative of bacterial infection with organ dysfunction (cardiac, respiratory, renal, or hematologic). Multivariable logistic regression was used to measure association of race/ethnicity, insurance status, and social disorganization index, with the primary outcome of mortality, adjusting for age, sex, complex chronic conditions, organ dysfunction on day 1, source of admission, and time to hospital. Secondary outcomes were ICU admission, readmission, organ dysfunction-free days, and sepsis therapies.
Results: Among 4532 patient episodes, the mortality rate was 9.7%. There was no difference in adjusted odds of mortality on the basis of race/ethnicity, insurance status, or social disorganization. There was no significant association between our predictors and ICU admission. Hispanic patients and publicly insured patients were more likely to be readmitted within 1 year (Hispanic odds ratio 1.28 [1.06-1.5]; public odds ratio 1.19 [1.05-1.35]).
Conclusions: Previously described disparities were not observed when using electronic clinical data to identify sepsis; however, data were only single center. There were significantly higher readmissions in patients who were publicly insured or identified as Hispanic or Latino, which require further investigation.
Copyright © 2023 by the American Academy of Pediatrics.
Conflict of interest statement
Figures
Similar articles
-
Hospital outcomes for children with severe sepsis in the USA by race or ethnicity and insurance status: a population-based, retrospective cohort study.Lancet Child Adolesc Health. 2021 Feb;5(2):103-112. doi: 10.1016/S2352-4642(20)30341-2. Epub 2020 Dec 14. Lancet Child Adolesc Health. 2021. PMID: 33333071 Free PMC article.
-
Prehospital Sepsis Recognition and Outcomes for Patients with Sepsis by Race and Ethnicity.Prehosp Emerg Care. 2024;28(7):898-904. doi: 10.1080/10903127.2023.2294269. Epub 2023 Dec 22. Prehosp Emerg Care. 2024. PMID: 38095600
-
Disparities in Obstetric Readmissions: A Multistate Analysis, 2007-2014.Am J Perinatol. 2022 Jan;39(2):125-133. doi: 10.1055/s-0041-1739310. Epub 2021 Nov 10. Am J Perinatol. 2022. PMID: 34758500
-
Disparities in COVID-19 Outcomes by Race, Ethnicity, and Socioeconomic Status: A Systematic-Review and Meta-analysis.JAMA Netw Open. 2021 Nov 1;4(11):e2134147. doi: 10.1001/jamanetworkopen.2021.34147. JAMA Netw Open. 2021. PMID: 34762110 Free PMC article.
-
Is Our Science Representative? A Systematic Review of Racial and Ethnic Diversity in Orthopaedic Clinical Trials from 2000 to 2020.Clin Orthop Relat Res. 2022 May 1;480(5):848-858. doi: 10.1097/CORR.0000000000002050. Epub 2021 Dec 2. Clin Orthop Relat Res. 2022. PMID: 34855650 Free PMC article.
References
-
- Czaja AS, Zimmerman JJ, Nathens AB. Readmission and late mortality after pediatric severe sepsis. Pediatrics 2009;123(3):849–857. - PubMed
-
- Ruth A, McCracken CE, Fortenberry JD, Hall M, Simon HK, Hebbar KB. Pediatric severe sepsis: current trends and outcomes from the Pediatric Health Information Systems database. Pediatric Critical Care Medicine 2014;15(9):828–838. - PubMed
-
- Hartman ME, Linde-Zwirble WT, Angus DC, Watson RS. Trends in the epidemiology of pediatric severe sepsis*. Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies 2013;14(7):686–693. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
