

Cost-effectiveness analysis of cardiac implantable electronic devices with reactive atrial-based antitachycardia pacing
- PMID: 36691793
- PMCID: PMC10062312
- DOI: 10.1093/europace/euad003
Cost-effectiveness analysis of cardiac implantable electronic devices with reactive atrial-based antitachycardia pacing
Abstract
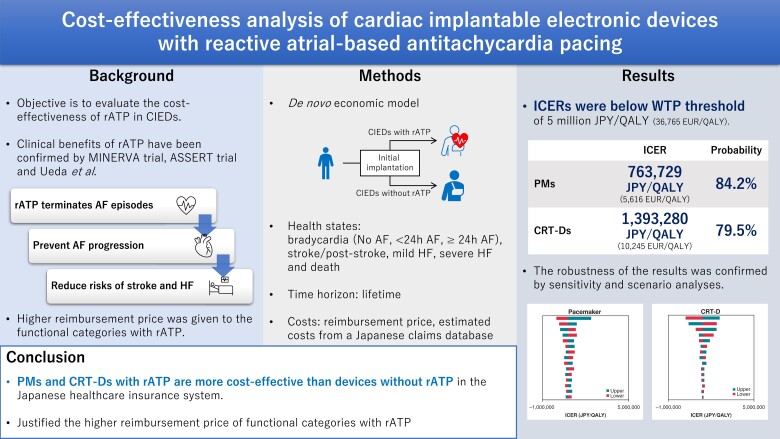
Aims: Reactive atrial-based anti-tachycardia pacing (rATP) in pacemakers (PMs) and cardiac resynchronization therapy defibrillators (CRT-Ds) has been reported to prevent progression of atrial fibrillation, and this reduced progression is expected to decrease the risk of complications such as stroke and heart failure (HF). This study aimed to assess the cost-effectiveness of rATP in PMs and CRT-Ds in the Japanese public health insurance system.
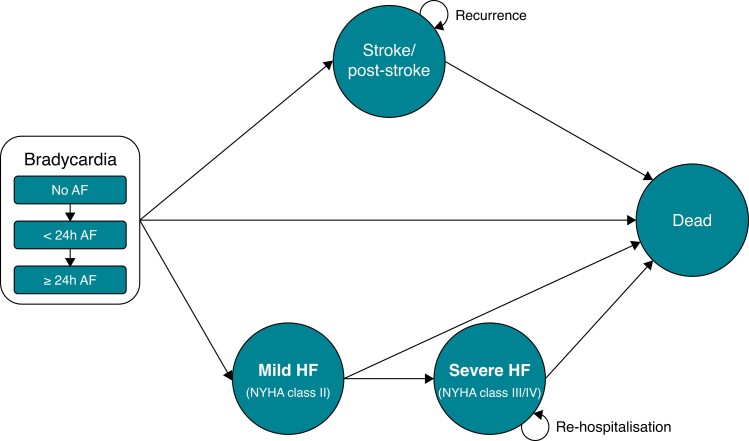
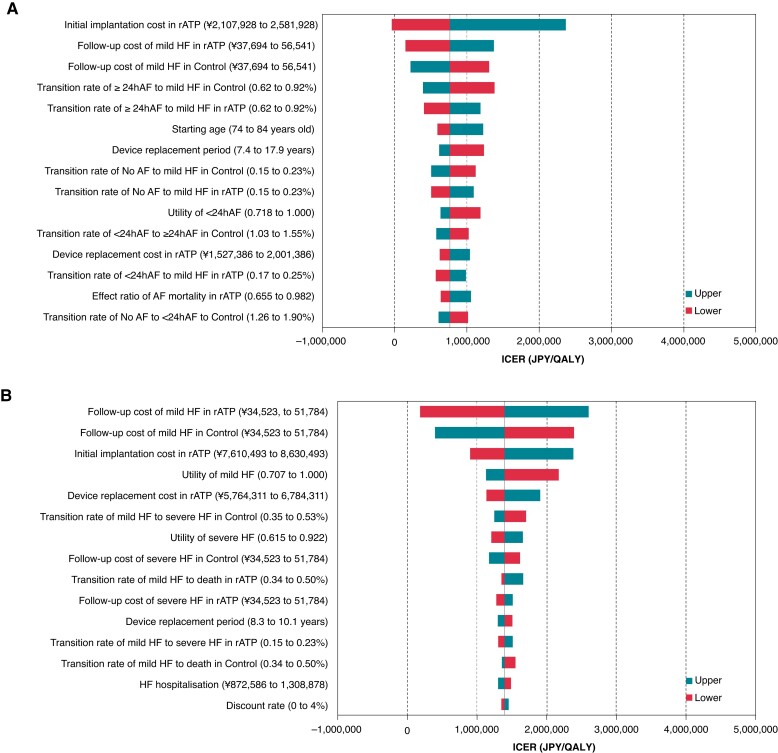
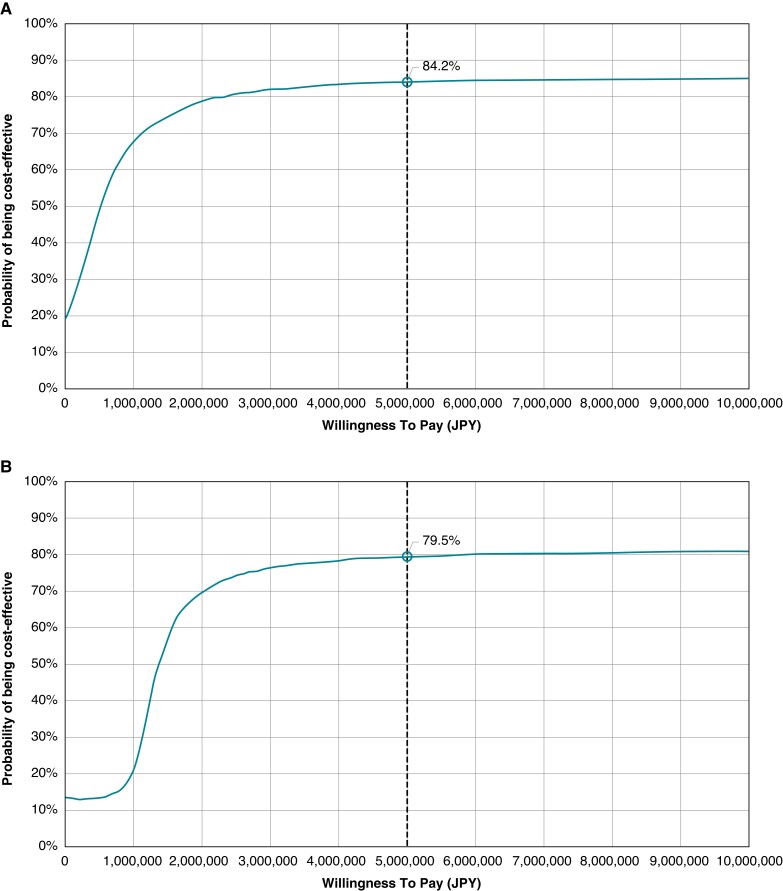
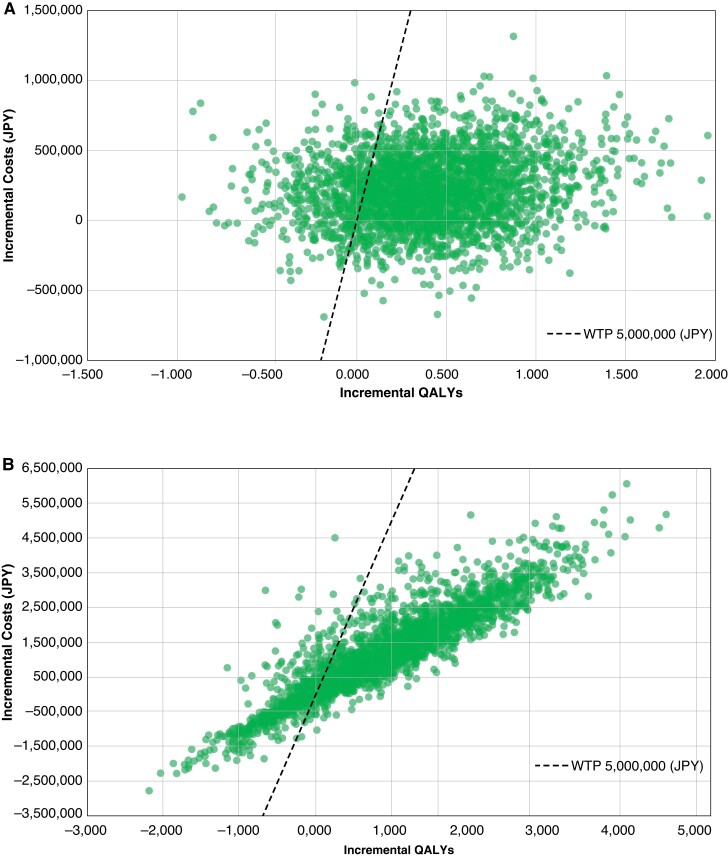
Methods and results: We developed a Markov model comprising five states: bradycardia, post-stroke, mild HF, severe HF, and death. For devices with rATP and control devices without rATP, we compared the incremental cost-effectiveness ratio (ICER) from the payer's perspective. Costs were estimated from healthcare resource utilisation data in a Japanese claims database. We evaluated model uncertainty by analysing two scenarios for each device. The ICER was 763 729 JPY/QALY (5616 EUR/QALY) for PMs and 1,393 280 JPY/QALY (10 245 EUR/QALY) for CRT-Ds. In all scenarios, ICERs were below 5 million JPY/QALY (36 765 EUR/QALY), supporting robustness of the results.
Conclusion: According to a willingness to pay threshold of 5 million JPY/QALY, the devices with rATP were cost-effective compared with control devices without rATP, showing that the higher reimbursement price of the functional categories with rATP is justified from a healthcare economic perspective.
Keywords: Atrial anti-tachycardia pacing; Atrial fibrillation; Cardiac resynchronization therapy; Cost-effectiveness; Heart failure; Pacemaker.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: Y.T., Y.I., and T.M. are employees of Medtronic Japan, and J.-E.M. is an employee of Medtronic Korea. T.U., H.Y., and A.S. are employees of Medilead, which was commissioned by Medtronic Japan. K.K., T.N., and N.U. have received compensation for advisory services for this study from Medtronic Japan and other payments, including honoraria, for lectures which were not directly associated with this study from Medtronic Japan. K.K. has received speaker honoraria from Medtronic Japan, Biotronik Japan and Boston Scientific and research grants from Medtronic Japan and Biotronik Japan. The authors have no other conflicts of interest to disclose.
Figures
Similar articles
-
Cost-effectiveness analyses to assess the value of reactive atrial-based anti-tachycardia pacing for patients with pacemakers and defibrillators: An Australian private healthcare system perspective.J Arrhythm. 2025 Apr 23;41(2):e70043. doi: 10.1002/joa3.70043. eCollection 2025 Apr. J Arrhythm. 2025. PMID: 40271387 Free PMC article.
-
Economic Value and Cost-Effectiveness of Cardiac Resynchronization Therapy Among Patients With Mild Heart Failure: Projections From the REVERSE Long-Term Follow-Up.JACC Heart Fail. 2017 Mar;5(3):204-212. doi: 10.1016/j.jchf.2016.10.014. Epub 2017 Jan 11. JACC Heart Fail. 2017. PMID: 28254126
-
Economic Considerations of Cardiovascular Implantable Electronic Devices for The Treatment of Heart Failure.Curr Heart Fail Rep. 2024 Jun;21(3):186-193. doi: 10.1007/s11897-024-00664-y. Epub 2024 Apr 25. Curr Heart Fail Rep. 2024. PMID: 38662154 Review.
-
Reactive atrial-based antitachycardia pacing therapy reduces atrial tachyarrhythmias.Pacing Clin Electrophysiol. 2019 Jul;42(7):970-979. doi: 10.1111/pace.13696. Epub 2019 Apr 29. Pacing Clin Electrophysiol. 2019. PMID: 30977146 Free PMC article.
-
A review of economic evaluation models for cardiac resynchronization therapy with implantable cardioverter defibrillators in patients with heart failure.Eur J Health Econ. 2016 Dec;17(9):1159-1172. doi: 10.1007/s10198-015-0752-3. Epub 2016 Jan 4. Eur J Health Econ. 2016. PMID: 26728985 Free PMC article. Review.
Cited by
-
Cost-effectiveness analyses to assess the value of reactive atrial-based anti-tachycardia pacing for patients with pacemakers and defibrillators: An Australian private healthcare system perspective.J Arrhythm. 2025 Apr 23;41(2):e70043. doi: 10.1002/joa3.70043. eCollection 2025 Apr. J Arrhythm. 2025. PMID: 40271387 Free PMC article.
References
-
- Inoue H, Fujiki A, Origasa H, Ogawa S, Okumura K, Kubota Iet al. . Prevalence of atrial fibrillation in the general population of Japan: an analysis based on periodic health examination. Int J Cardiol 2009;137:102–7. - PubMed
-
- National Federation of Health Insurance Societies (KENPOREN) . Trend survey on the top 30 diseases in medical expenses in January 2022. (in Japanese). https://www.kenporen.com/toukei_data/pdf/chosa_r04_06_05.pdf
-
- Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DLet al. . 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation [published correction appears in Eur Heart J. 2021 May 14; 42(19):1908] [published correction appears in Eur Heart J. 2021 May 14; 42(19):1925] [published correction appears in Eur Heart J. 2021 May 13]. Eur Heart J 2021;42:1289–367. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
