

Epstein-Barr virus-associated primary intracranial leiomyosarcoma in an immunocompetent patient: illustrative case
- PMID: 36692065
- PMCID: PMC10550697
- DOI: 10.3171/CASE22532
Epstein-Barr virus-associated primary intracranial leiomyosarcoma in an immunocompetent patient: illustrative case
Abstract
Background: Primary intracranial leiomyosarcomas (PILMSs) are extremely rare tumors arising from smooth muscle connective tissue. PILMSs have been shown to be associated with Epstein-Barr virus (EBV). Thus far, EBV-associated PILMS has been exclusively described in immunocompromised patients.
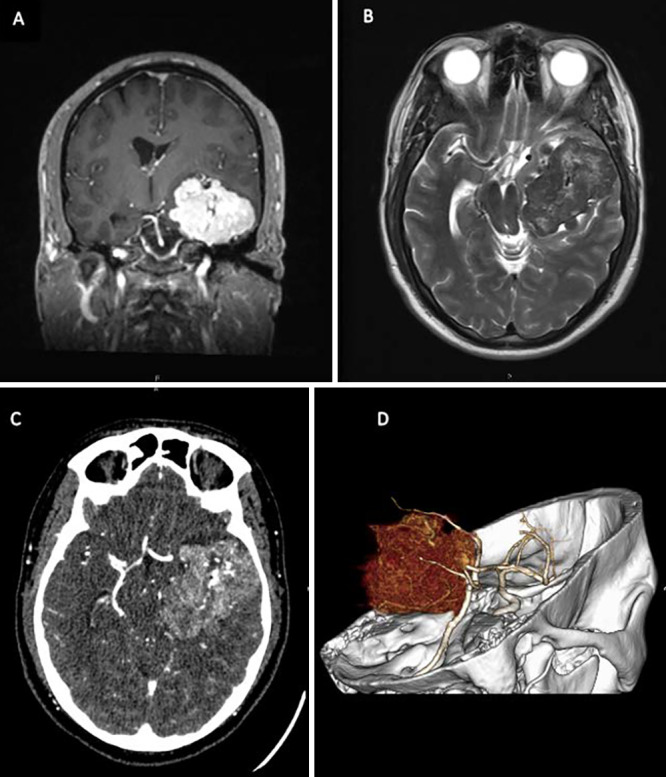
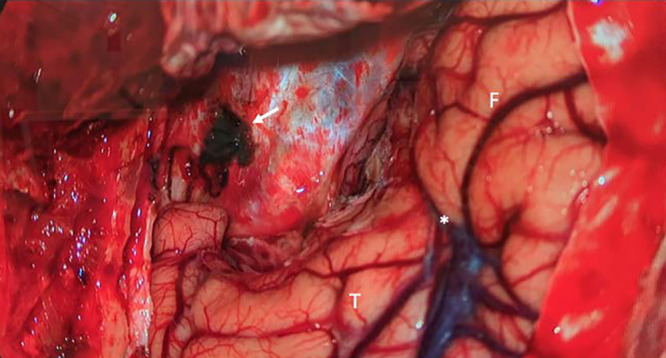
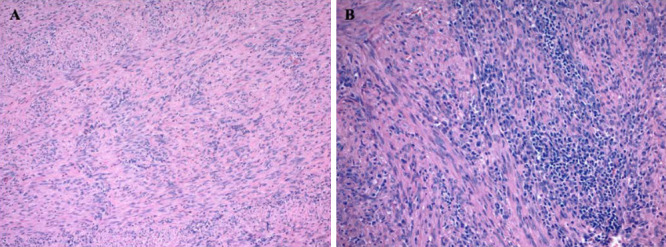
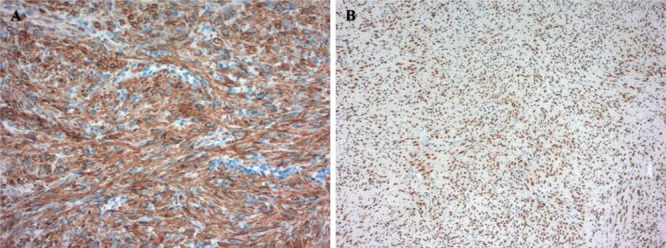
Observations: A 40-year-old male presented with a 2-year history of left-sided headaches, nausea, and vomiting. Magnetic resonance imaging demonstrated a large, heterogeneously enhancing, lobulated, dura-based mass arising from the left middle cranial fossa with associated edema and mass effect. The patient underwent an uncomplicated resection of suspected meningioma; neuropathology revealed the exceedingly rare diagnosis of EBV-associated PILMS. Follow-up testing for human immunodeficiency virus (HIV) and other immunodeficiencies confirmed the patient's immunocompetent status.
Lessons: Primary intracranial smooth muscle tumors are often misdiagnosed as meningiomas due to their similar appearance on imaging. PILMSs have a poor prognosis and gross total resection is the mainstay of treatment in the absence of clear recommendations for management. Prompt diagnosis and resection are important; therefore, these tumors should be included in the differential of dura-based tumors, especially among immunocompromised patients. Although EBV-associated PILMSs usually occur in immunocompromised individuals, their presence cannot be ruled out in immunocompetent patients.
Keywords: Epstein-Barr virus; immunocompetent; primary intracranial leiomyosarcoma; sarcoma; smooth muscle tumor.
Conflict of interest statement
Figures
Similar articles
-
EBV-associated leiomyosarcoma in an immunocompromised child: A unique intracranial case with genomic study.Int J Surg Case Rep. 2025 Mar;128:111073. doi: 10.1016/j.ijscr.2025.111073. Epub 2025 Feb 18. Int J Surg Case Rep. 2025. PMID: 40024176 Free PMC article.
-
Concurrent occurrence of primary intracranial Epstein-Barr virus-associated leiomyosarcoma and Hodgkin lymphoma in a young adult.J Neurosurg. 2013 Aug;119(2):499-503. doi: 10.3171/2013.3.JNS121707. Epub 2013 Apr 26. J Neurosurg. 2013. PMID: 23621602
-
Latent Epstein-Barr virus infection demonstrated in low-grade leiomyosarcomas of adults with acquired immunodeficiency syndrome, but not in adjacent Kaposi's lesion or smooth muscle tumors in immunocompetent patients.Arch Pathol Lab Med. 1997 Aug;121(8):834-8. Arch Pathol Lab Med. 1997. PMID: 9278611
-
Primary meningeal Epstein-Barr virus-related leiomyosarcoma in a man infected with human immunodeficiency virus: review of literature, emphasizing the differential diagnosis and pathogenesis.Appl Immunohistochem Mol Morphol. 2004 Dec;12(4):387-91. doi: 10.1097/00129039-200412000-00018. Appl Immunohistochem Mol Morphol. 2004. PMID: 15536343 Review.
-
Primary intracranial leiomyosarcoma in an HIV-infected patient.Int J Clin Oncol. 2011 Feb;16(1):63-6. doi: 10.1007/s10147-010-0110-5. Epub 2010 Jul 30. Int J Clin Oncol. 2011. PMID: 20676716 Review.
Cited by
-
EBV-associated leiomyosarcoma in an immunocompromised child: A unique intracranial case with genomic study.Int J Surg Case Rep. 2025 Mar;128:111073. doi: 10.1016/j.ijscr.2025.111073. Epub 2025 Feb 18. Int J Surg Case Rep. 2025. PMID: 40024176 Free PMC article.
-
Giant primary intracranial multi-fossa leiomyosarcoma involving the frontal sinus, ethmoid air cells, anterior fossa, middle fossa, and intraventricular space: A case report and literature review.Surg Neurol Int. 2023 Oct 27;14:384. doi: 10.25259/SNI_647_2023. eCollection 2023. Surg Neurol Int. 2023. PMID: 37941634 Free PMC article.
-
A Clinicopathology Review and Update of Epstein-Barr Virus-Associated Mesenchymal Tumors.Cancers (Basel). 2023 Nov 24;15(23):5563. doi: 10.3390/cancers15235563. Cancers (Basel). 2023. PMID: 38067267 Free PMC article. Review.
References
-
- Singh Z. Leiomyosarcoma: a rare soft tissue cancer arising from multiple organs. J Cancer Res Pract. 2018;5(1):1–8.
-
- Paulus W, Slowik F, Jellinger K. Primary intracranial sarcomas: histopathological features of 19 cases. Histopathology. 1991;18(5):395–402. - PubMed
-
- Aeddula NR, Pathireddy S, Samaha T, Ukena T, Hosseinnezhad A. Primary intracranial leiomyosarcoma in an immunocompetent adult. J Clin Oncol. 2011;29(14):e407–e410. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
