

Review
doi: 10.1148/radiol.222379.
Epub 2023 Jan 24.
Chronic Pulmonary Manifestations of COVID-19 Infection: Imaging Evaluation
Affiliations
- PMID: 36692398
- PMCID: PMC9888022
- DOI: 10.1148/radiol.222379
Item in Clipboard
Review
Chronic Pulmonary Manifestations of COVID-19 Infection: Imaging Evaluation
Radiology.
2023 Apr.
Abstract
This case presents a patient with severe COVID-19 pneumonia requiring intensive care unit admission and a prolonged hospital stay. The infection resulted in long-term morbidity, functional decline, and abnormal chest CT findings. The mechanisms for long-term lung injury after COVID-19 infection, imaging appearances, and the role of imaging in follow-up are discussed.
© RSNA, 2023.
Conflict of interest statement
Figures

Dr Murphy completed radiology residency in the Mater
Misericordiae University Hospital in Dublin, Ireland. He is currently
undertaking a fellowship in cardiothoracic imaging and intervention at
Massachusetts General Hospital, Boston, where he was awarded a Ralph
Schlaeger grant for research activities.

Dr Little is a cardiothoracic radiologist at Mayo Clinic,
Florida. His clinical and research interests include imaging of COVID-19 and
other infections, diffuse lung disease, and lung cancer screening. He also
has a longstanding interest in radiology teaching and education.

A 51-year-old man with COVID-19 infection. Anteroposterior chest radiograph
shows extensive pulmonary opacities bilaterally with a lower lung and
peripheral predominance.
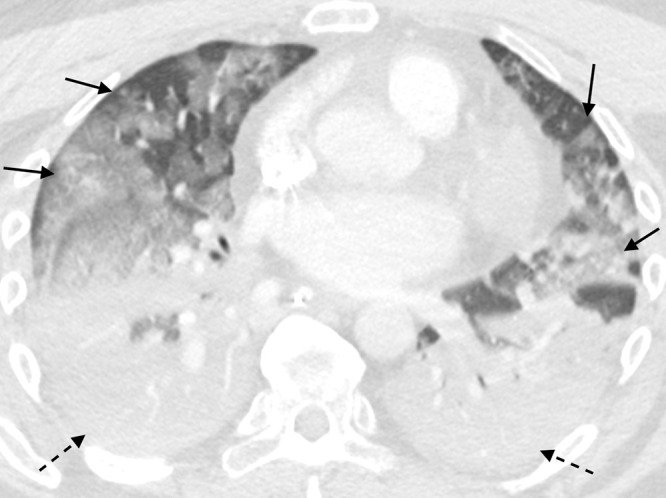
A 51-year-old man with COVID-19 infection. Axial contrast-enhanced CT image
obtained the week of initial presentation after intensive care unit
transfer. There is dense consolidation within the dependent portions of the
lungs bilaterally (dashed arrows) and multifocal ground-glass opacity within
the nondependent portions of the lungs (solid arrows). These findings are
suggestive of a diffuse alveolar damage pattern of lung injury.
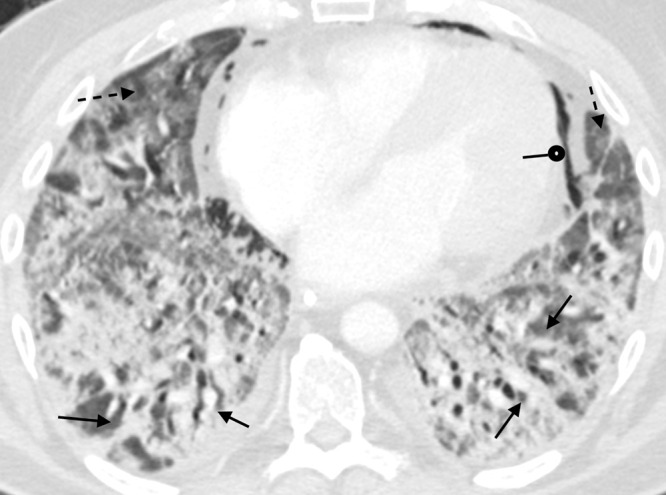
A 51-year-old man with COVID-19 infection. Axial contrast-enhanced CT image
obtained 1 month after initial presentation. There is improved aeration of
the dependent portions of the lungs; however, there is residual
consolidation with contraction and architectural distortion (solid arrows).
There is also persistent ground-glass opacity (dashed arrows) and new
bronchial dilatation bilaterally. This appearance is suggestive of the
organizing phase of acute lung injury. There is pneumomediastinum (round
arrow) likely secondary to barotrauma from mechanical ventilation.
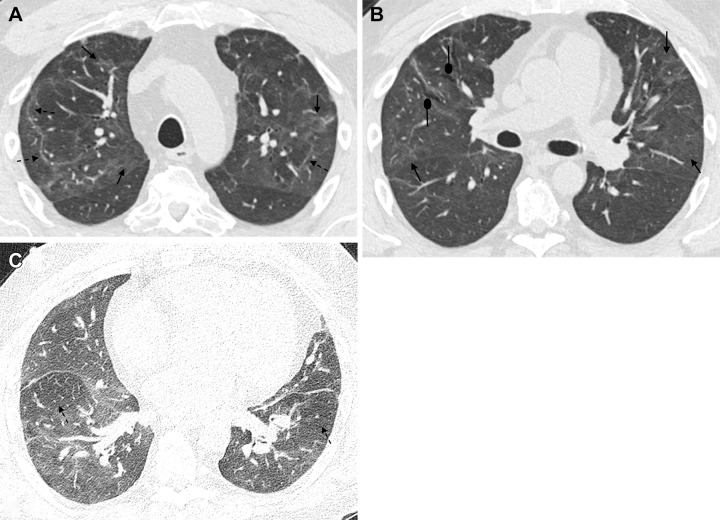
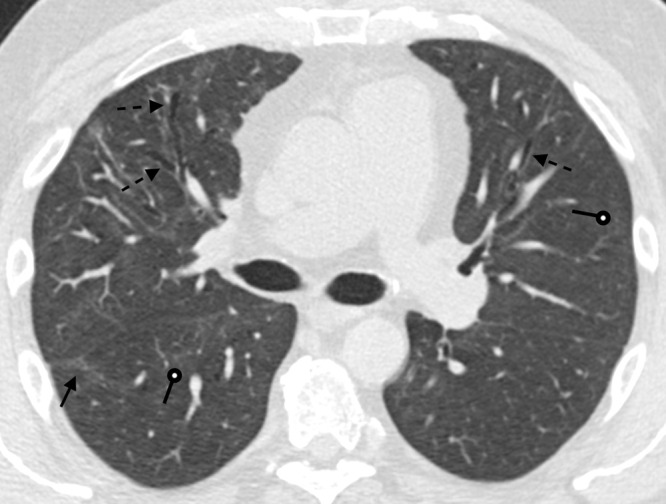
A 51-year-old man 6 months after COVID-19 infection. Axial contrast-enhanced
CT images from a series obtained at (A, B) inspiration and
(C) expiration. (A) Persistent faint
ground-glass opacities scattered throughout the lung parenchyma (solid
arrows) have decreased in attenuation since prior imaging but remain
extensive (tinted sign). Subpleural curvilinear opacities represent
parenchymal bands and perilobular opacities (dashed arrows).
(B) Mild anterior varicose bronchiectasis appreciated
anteriorly in the right middle lobe (round arrows). Faint persistent
ground-glass opacities (solid arrows). (C) Lobular and regional
areas of persistent low attenuation (dashed arrows) on expiratory images
consistent with air trapping, suggestive of small airway disease.
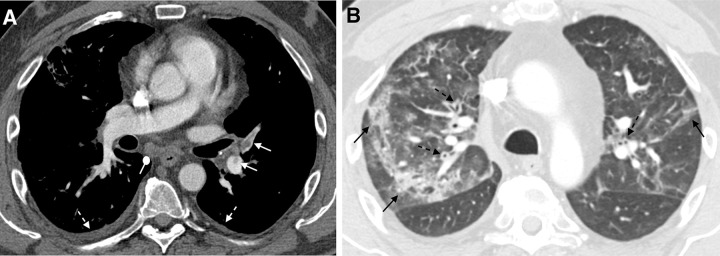
A 51-year-old man 6 months after COVID-19 infection with shortness of breath.
Axial CT pulmonary angiograms obtained with (A) soft-tissue and
(B) lung window settings at second acute presentation to
the emergency department. There are filling defects within several pulmonary
artery branches (solid white arrows), consistent with acute pulmonary
emboli. Multifocal patchy and linear ground-glass opacities and
consolidation (solid black arrows) are new from 2 weeks prior. New bronchial
wall thickening (dashed black arrows) and bilateral small pleural effusions
(dashed white arrows). These findings suggest a superimposed acute
process.
A 51-year-old man 9 months after COVID-19 infection. Axial contrast-enhanced
CT image shows mild persistent anterior varicose bronchiectasis and
architectural distortion best appreciated in the right middle lobe (dashed
arrows). Faint patchy ground-glass opacities and reticulation are improved
from 6-month imaging and barely perceptible (round arrows). Faint linear
parenchymal bands have greatly improved (solid arrow). This may reflect the
patient's new baseline.

A 60-year-old woman with a history of hospitalization for moderate
COVID-19 pneumonia requiring supplemental oxygen but not mechanical
ventilation. Axial noncontrast CT image obtained 25 months after
presentation for COVID-19 pneumonia shows bilateral thin parenchymal
bands (white arrows), peripheral reticulation (black arrows), patchy
ground-glass attenuation and reticulation, and traction bronchiectasis
with architectural distortion (dashed black arrows). The fibrotic-like
findings shown here appear to represent a new baseline given the 2-year
period and have a pattern suggesting fibrotic sequelae of organizing
lung injury in the setting of COVID-19. In other cases, parenchymal
bands, ground-glass opacities, reticulation, and bronchial dilatation
improve or resolve at follow-up imaging and cannot be interpreted as
irreversible fibrosis without follow-up imaging.
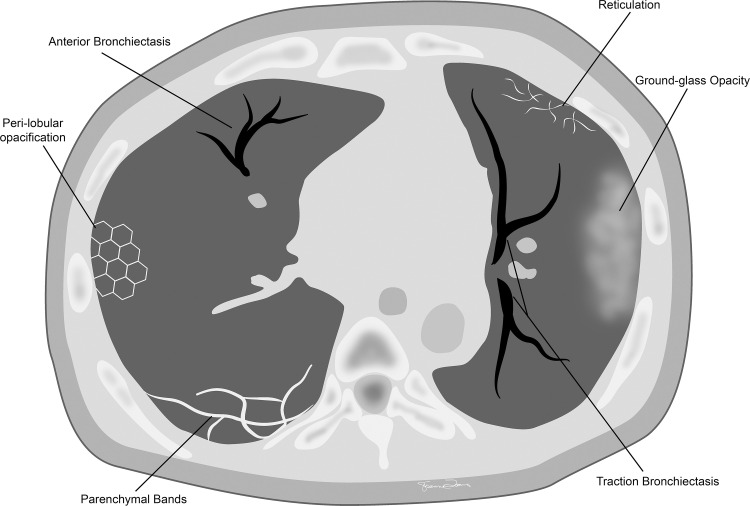
Commonly seen chronic CT findings after COVID-19 infection.
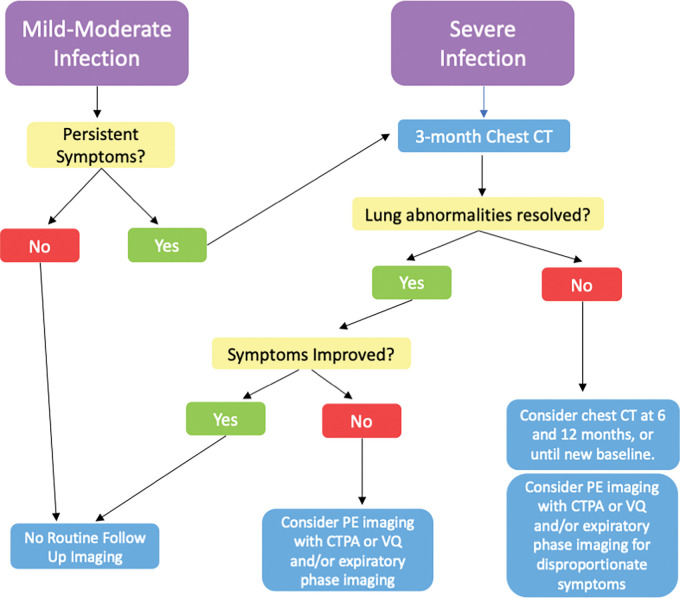
Flowchart shows the timing of imaging follow-up and the role of imaging
modalities after COVID-19 infection. CTPA = CT pulmonary angiography, PE
= pulmonary embolus, V/Q = ventilation-perfusion.
Similar articles
-
Clinical manifestations and radiological features by chest computed tomographic findings of a novel coronavirus disease-19 pneumonia among 92 patients in Japan.J Microbiol Immunol Infect. 2021 Aug;54(4):748-751. doi: 10.1016/j.jmii.2020.07.011. Epub 2020 Aug 20. J Microbiol Immunol Infect. 2021. PMID: 32868193 Free PMC article.
-
Analysis of thin-section CT in patients with coronavirus disease (COVID-19) after hospital discharge.J Xray Sci Technol. 2020;28(3):383-389. doi: 10.3233/XST-200685. J Xray Sci Technol. 2020. PMID: 32474479 Free PMC article.
-
Are the thorax Computed Tomography findings of ICU patients diagnosed with COVID-19 pneumonia related to the duration of hospital stay and mortality?J Infect Chemother. 2023 May;29(5):495-501. doi: 10.1016/j.jiac.2022.12.016. Epub 2023 Jan 7. J Infect Chemother. 2023. PMID: 36627082 Free PMC article.
-
Role of computed tomography in COVID-19.J Cardiovasc Comput Tomogr. 2021 Jan-Feb;15(1):27-36. doi: 10.1016/j.jcct.2020.08.013. Epub 2020 Sep 4. J Cardiovasc Comput Tomogr. 2021. PMID: 32952101 Free PMC article. Review.
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2020 Sep 30;9:CD013639. doi: 10.1002/14651858.CD013639.pub2. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2020 Nov 26;11:CD013639. doi: 10.1002/14651858.CD013639.pub3. PMID: 32997361 Updated.
Cited by
-
Effects of sulphur thermal water inhalations in long-COVID syndrome: Spa-centred, double-blinded, randomised case-control pilot study.Clin Med (Lond). 2024 Nov;24(6):100251. doi: 10.1016/j.clinme.2024.100251. Epub 2024 Oct 5. Clin Med (Lond). 2024. PMID: 39370044 Free PMC article. Clinical Trial.
-
Long-Term Effects of COVID-19: Analysis of Imaging Findings in Patients Evaluated by Computed Tomography from 2020 to 2024.Tomography. 2025 Apr 24;11(5):49. doi: 10.3390/tomography11050049. Tomography. 2025. PMID: 40423251 Free PMC article.
-
Residual radiological opacities correlate with disease outcomes in ICU-treated COVID-19.Front Med (Lausanne). 2024 Apr 3;11:1263511. doi: 10.3389/fmed.2024.1263511. eCollection 2024. Front Med (Lausanne). 2024. PMID: 38633311 Free PMC article.
-
MMP-9 metalloproteinase and its regulator are not associated with mid-term CT residual abnormalities in patients with COVID-19 pneumonia.Acta Radiol Open. 2025 Apr 16;14(4):20584601251330563. doi: 10.1177/20584601251330563. eCollection 2025 Apr. Acta Radiol Open. 2025. PMID: 40291835 Free PMC article.
-
Detection of Severe Lung Infection on Chest Radiographs of COVID-19 Patients: Robustness of AI Models across Multi-Institutional Data.Diagnostics (Basel). 2024 Feb 5;14(3):341. doi: 10.3390/diagnostics14030341. Diagnostics (Basel). 2024. PMID: 38337857 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
