

Laparoscopy in high-risk emergency general surgery reduces intensive care stay, length of stay and mortality
- PMID: 36692646
- PMCID: PMC9872062
- DOI: 10.1007/s00423-022-02744-w
Laparoscopy in high-risk emergency general surgery reduces intensive care stay, length of stay and mortality
Abstract
Purpose: Emergency general surgery patients undergoing laparoscopic surgery are at reduced risk of mortality and may require reduced length of critical care stay. This study investigated the effect of laparoscopy on high-risk patients' post-operative care requirements.
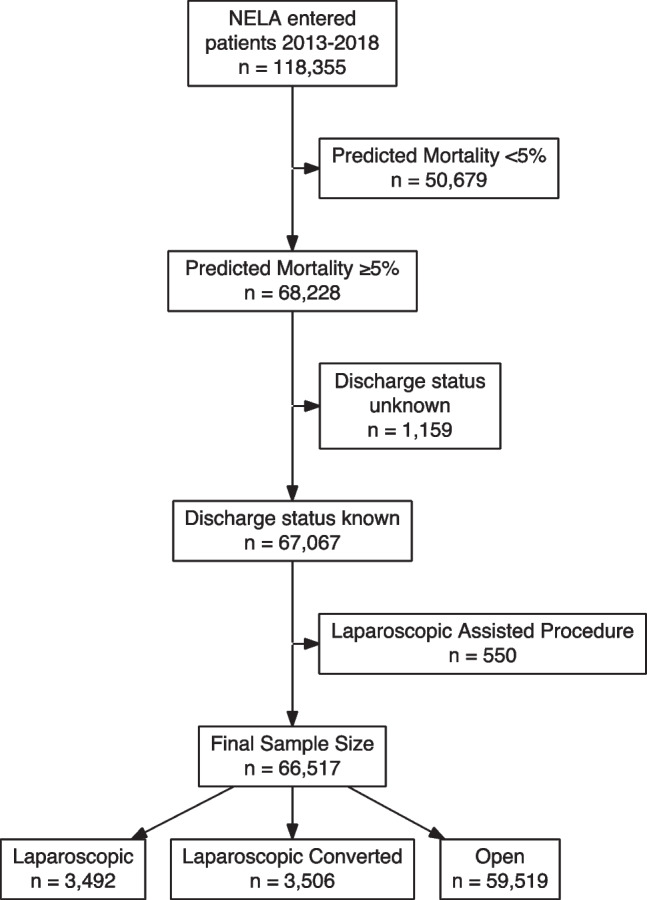
Methods: Data were retrieved for all patients entered into the NELA database between 2013 and 2018. Only high-risk surgical patients (P-POSSUM predicted mortality risk of ≥ 5%) were included. Patients undergoing laparoscopic and open emergency general surgical procedures were compared using a propensity score weighting approach. Outcome measures included total length of critical care (level 3) stay, overall length of stay and inpatient mortality.
Results: A total of 66,517 high-risk patients received emergency major abdominal surgery. A laparoscopic procedure was attempted in 6998 (10.5%); of these, the procedure was competed laparoscopically in 3492 (49.9%) and converted to open in 3506 (50.1%). Following inverse probability treatment weighting adjustment for patient disease and treatment characteristics, high-risk patients undergoing laparoscopic surgery had a shorter median ICU stay (1 day vs 2 days p < 0.001), overall hospital length of stay (11 days vs 14 days p < 0.001) and a lower inpatient mortality (16.0% vs 18.8%, p < 0.001). They were also less likely to have a prolonged ICU stay with an OR of 0.78 (95% CI 0.74-0.83, p < 0.001).
Conclusion: The results of this study suggest that in patients at high risk of post-operative mortality, laparoscopic emergency bowel surgery leads to a reduced length of critical care stay, overall length of stay and inpatient mortality compared to traditional laparotomy.
Keywords: Critical care; Emergency general surgery; Laparoscopy.
© 2023. The Author(s), under exclusive licence to Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Similar articles
-
A national propensity score-matched analysis of emergency laparoscopic versus open abdominal surgery.Br J Surg. 2021 Aug 19;108(8):934-940. doi: 10.1093/bjs/znab048. Br J Surg. 2021. PMID: 33724351 Free PMC article.
-
P-POSSUM and the NELA Score Overpredict Mortality for Laparoscopic Emergency Bowel Surgery: An Analysis of the NELA Database.World J Surg. 2022 Mar;46(3):552-560. doi: 10.1007/s00268-021-06404-w. Epub 2022 Jan 10. World J Surg. 2022. PMID: 35001139
-
Assessing outcomes in laparoscopic vs open surgical management of adhesive small bowel obstruction.Surg Endosc. 2023 Feb;37(2):1376-1383. doi: 10.1007/s00464-022-09314-7. Epub 2022 May 19. Surg Endosc. 2023. PMID: 35587296
-
Laparoscopic versus open approach for adhesive small bowel obstruction, a systematic review and meta-analysis of short term outcomes.J Trauma Acute Care Surg. 2020 Jun;88(6):866-874. doi: 10.1097/TA.0000000000002684. J Trauma Acute Care Surg. 2020. PMID: 32195994
-
Effect of sarcopenia in predicting postoperative mortality in emergency laparotomy: a systematic review and meta-analysis.World J Emerg Surg. 2022 Jun 25;17(1):36. doi: 10.1186/s13017-022-00440-0. World J Emerg Surg. 2022. PMID: 35752855 Free PMC article.
Cited by
-
Minimally invasive approach to peritonitis from left colonic perforation: a retrospective multicenter observational study.Surg Endosc. 2025 Apr;39(4):2370-2379. doi: 10.1007/s00464-025-11611-w. Epub 2025 Feb 18. Surg Endosc. 2025. PMID: 39966134 Free PMC article.
-
Trends in Clinical Outcomes After Major Emergency Abdominal Surgery in Denmark, Data From 2002-2022.JAMA Surg. 2025 Jun 1;160(6):665-673. doi: 10.1001/jamasurg.2025.0858. JAMA Surg. 2025. PMID: 40266626
-
Open versus laparoscopic completion cholecystectomy in patients with previous open partial cholecystectomy: a retrospective comparative study.Ann Med Surg (Lond). 2024 Aug 6;86(10):5688-5695. doi: 10.1097/MS9.0000000000002428. eCollection 2024 Oct. Ann Med Surg (Lond). 2024. PMID: 39359822 Free PMC article.
-
Cesena guidelines: WSES consensus statement on laparoscopic-first approach to general surgery emergencies and abdominal trauma.World J Emerg Surg. 2023 Dec 8;18(1):57. doi: 10.1186/s13017-023-00520-9. World J Emerg Surg. 2023. PMID: 38066631 Free PMC article.
-
European society for trauma and emergency surgery member-identified research priorities in emergency surgery: a roadmap for future clinical research opportunities.Eur J Trauma Emerg Surg. 2024 Apr;50(2):367-382. doi: 10.1007/s00068-023-02441-3. Epub 2024 Feb 27. Eur J Trauma Emerg Surg. 2024. PMID: 38411700 Free PMC article. Review.
References
-
- Principle standards reported by the National Emergency Laparotomy Audit (NELA). https://www.nela.org.uk/downloads/NELA%20standards.pdf
MeSH terms
LinkOut - more resources
Full Text Sources
