

Prevalence of Drug-Drug Interactions in Older Community-Dwelling Individuals: A Systematic Review and Meta-analysis
- PMID: 36692678
- PMCID: PMC9925489
- DOI: 10.1007/s40266-022-01001-5
Prevalence of Drug-Drug Interactions in Older Community-Dwelling Individuals: A Systematic Review and Meta-analysis
Abstract
Background: Drug-drug interactions (DDIs) can lead to medication-related harm, and the older population is at greatest risk. We conducted a systematic review and meta-analysis to estimate DDI prevalence and identify common DDIs in older community-dwelling adults.
Methods: PubMed and EMBASE were searched for observational studies published between 01/01/2010 and 10/05/2021 reporting DDI prevalence in community-dwelling individuals aged ≥ 65 years. Nursing home and inpatient hospital studies were excluded. Study quality was assessed using the Joanna Briggs Institute critical appraisal tool. Meta-analysis was performed using a random-effects model with logit transformation. Heterogeneity was evaluated using Cochran's Q and I2. DDI prevalence and 95% confidence intervals (CIs) are presented. All analyses were performed in R (version 4.1.2).
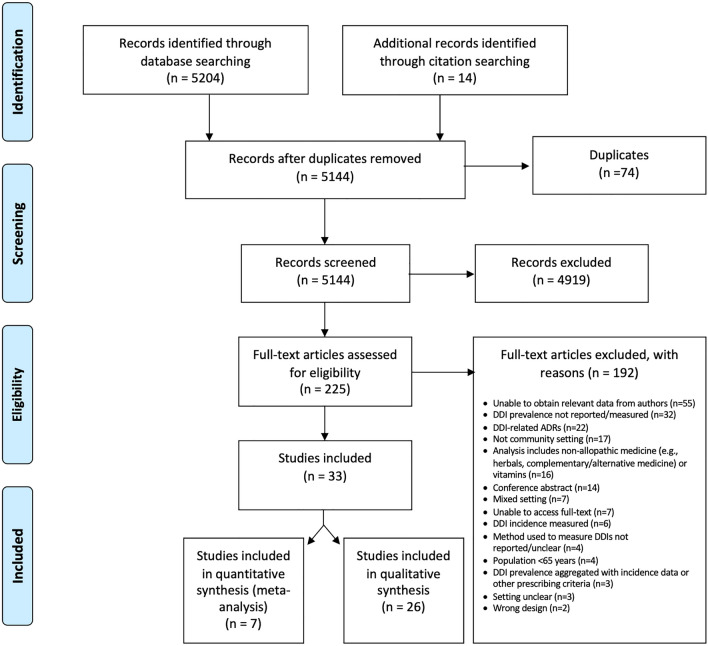
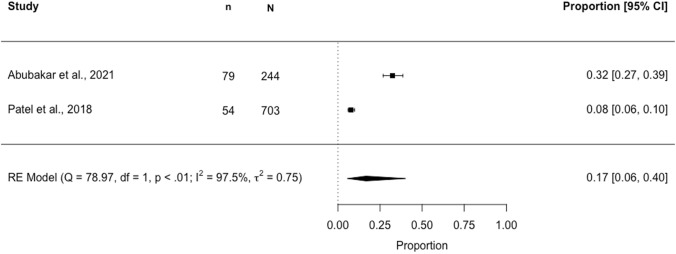
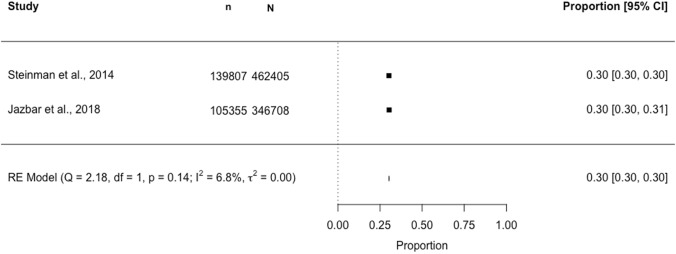
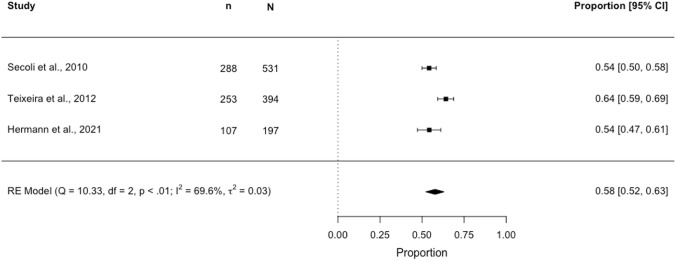
Results: There were 5144 unique articles identified. Thirty-three studies involving 17,011,291 community-dwelling individuals aged ≥ 65 years met inclusion criteria. Thirty-one studies reported DDI prevalence at the study-participant level, estimates ranged from 0.8% to 90.6%. The pooled DDI prevalence was 28.8% (95% CI 19.3-40.7), with significant heterogeneity (p < 0.10; I2 = 100%; tau2 = 2.13) largely explained by the different DDI identification methods. Therefore, 26 studies were qualitatively synthesised and seven studies were eligible for separate meta-analyses. In a meta-analysis of three studies (N = 1122) using Micromedex®, pooled DDI prevalence was 57.8% (95% CI 52.2-63.2; I2 = 69.6%, p < 0.01). In a meta-analysis of two studies (N = 809,113) using Lexi-Interact®, pooled DDI prevalence was 30.3% (95% CI 30.2-30.4; I2 = 6.8%). In a meta-analysis of two studies (N = 947) using the 2015 American Geriatrics Society Beers criteria®, pooled DDI prevalence was 16.6% (95% CI 5.6-40.2; I2 = 97.5%, p < 0.01). Common DDIs frequently involved cardiovascular drugs, including ACE inhibitor-potassium-sparing diuretic; amiodarone-digoxin; and amiodarone-warfarin.
Conclusions: DDIs are prevalent among older community-dwelling individuals; however, the methodology used to estimate these events varies considerably. A standardised methodology is needed to allow meaningful measurement and comparison of DDI prevalence.
© 2023. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest that are directly relevant to the content of this article.
Figures
Similar articles
-
The European Drug-Drug Interaction (EuroDDI) Study Protocol: A Cross-Country Comparison of Drug-Drug Interaction Prevalence in the Older Community-Dwelling Population.Pharmacoepidemiol Drug Saf. 2025 Jan;34(1):e70092. doi: 10.1002/pds.70092. Pharmacoepidemiol Drug Saf. 2025. PMID: 39777812 Free PMC article.
-
Drug-Drug Interactions and Their Association with Adverse Health Outcomes in the Older Community-Dwelling Population: A Prospective Cohort Study.Clin Drug Investig. 2024 Jun;44(6):439-453. doi: 10.1007/s40261-024-01369-9. Epub 2024 Jun 15. Clin Drug Investig. 2024. PMID: 38878216 Free PMC article.
-
Prevalence of clinically manifested drug interactions in hospitalized patients: A systematic review and meta-analysis.PLoS One. 2020 Jul 1;15(7):e0235353. doi: 10.1371/journal.pone.0235353. eCollection 2020. PLoS One. 2020. PMID: 32609783 Free PMC article.
-
Prevalence and Factors Associated with Potential Drug-Drug Interactions in Older Community-Dwelling Adults: A Prospective Cohort Study.Drugs Aging. 2021 Nov;38(11):1025-1037. doi: 10.1007/s40266-021-00898-8. Epub 2021 Oct 11. Drugs Aging. 2021. PMID: 34632551 Free PMC article.
-
Global Incidence of Frailty and Prefrailty Among Community-Dwelling Older Adults: A Systematic Review and Meta-analysis.JAMA Netw Open. 2019 Aug 2;2(8):e198398. doi: 10.1001/jamanetworkopen.2019.8398. JAMA Netw Open. 2019. PMID: 31373653 Free PMC article.
Cited by
-
The risk and cost of drug-drug interactions in an older population acutely admitted to hospital in Ireland.Int J Clin Pharm. 2025 Apr 10. doi: 10.1007/s11096-025-01907-1. Online ahead of print. Int J Clin Pharm. 2025. PMID: 40208397
-
Patterns, outcomes, and preventability of clinically manifest drug-drug interactions in older outpatients: a subgroup analysis from a 6-year-long observational study in North India.Naunyn Schmiedebergs Arch Pharmacol. 2025 Jan;398(1):687-698. doi: 10.1007/s00210-024-03294-2. Epub 2024 Jul 24. Naunyn Schmiedebergs Arch Pharmacol. 2025. PMID: 39046529
-
Potential Drug-Drug Interactions and Related Factors among Geriatric Outpatients of a Tertiary Care Hospital.Geriatrics (Basel). 2023 Nov 14;8(6):111. doi: 10.3390/geriatrics8060111. Geriatrics (Basel). 2023. PMID: 37987471 Free PMC article.
-
Polypharmacy, drug-drug interactions, anticholinergic burden and cognitive outcomes: a snapshot from a community-dwelling sample of older men and women in northern Italy.Eur J Ageing. 2024 Mar 29;21(1):11. doi: 10.1007/s10433-024-00806-0. Eur J Ageing. 2024. PMID: 38551689 Free PMC article.
-
The European Drug-Drug Interaction (EuroDDI) Study Protocol: A Cross-Country Comparison of Drug-Drug Interaction Prevalence in the Older Community-Dwelling Population.Pharmacoepidemiol Drug Saf. 2025 Jan;34(1):e70092. doi: 10.1002/pds.70092. Pharmacoepidemiol Drug Saf. 2025. PMID: 39777812 Free PMC article.
References
-
- The World Health Organization. WHO global patient safety challenge: medication without harm. 2017. http://apps.who.int/iris/bitstream/handle/10665/255263/WHO-HIS-SDS-2017..... Accessed 10 May 2021.
-
- Preston CL. Stockley's drug interactions: a source book of interactions, their mechanisms, clinical importance and management. 12. Pharmaceutical Press; 2019.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
