

A randomized controlled trial comparing femtosecond-enabled deep anterior lamellar keratoplasty and standard deep anterior lamellar keratoplasty (FEDS Study)
- PMID: 36693916
- PMCID: PMC10482827
- DOI: 10.1038/s41433-023-02387-1
A randomized controlled trial comparing femtosecond-enabled deep anterior lamellar keratoplasty and standard deep anterior lamellar keratoplasty (FEDS Study)
Abstract
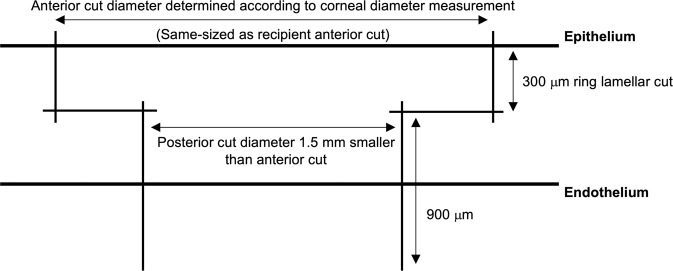
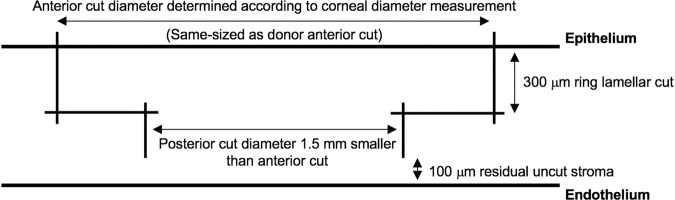
Objectives: To compare outcomes of femtosecond-enabled deep anterior lamellar keratoplasty (FE-DALK) and standard deep anterior lamellar keratoplasty (S-DALK).
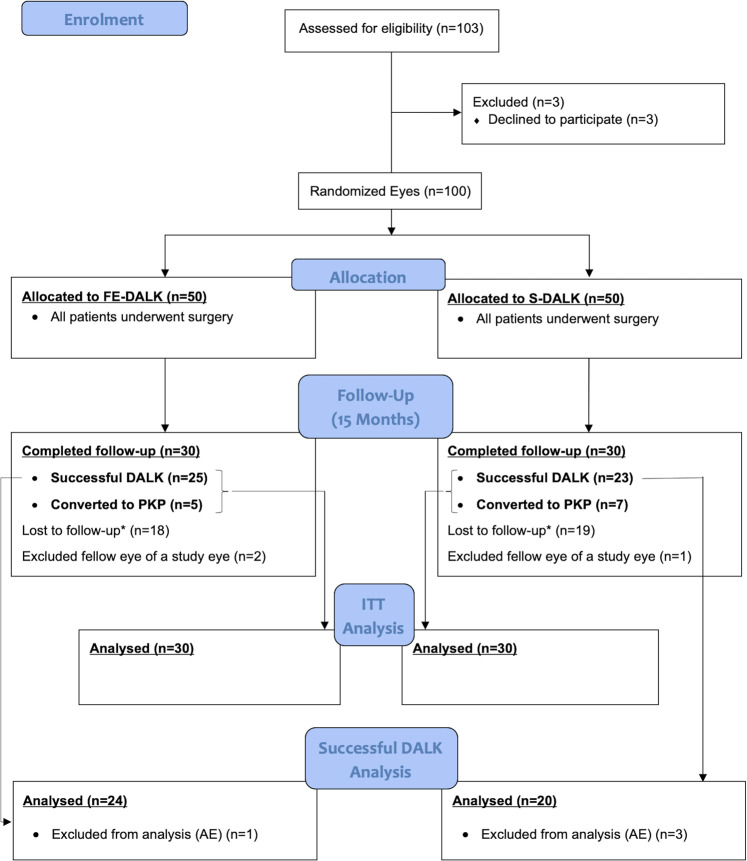
Methods: An open label, randomized controlled trial (Kensington Eye Institute, Toronto, ON, Canada) including 100 eyes of 97 participants with either keratoconus or corneal scarring, randomized to either FE-DALK (n = 48) or S-DALK (n = 49).
Primary outcomes: postoperative astigmatism and surgically induced corneal astigmatism (SIA) - both at 15 months.
Secondary outcomes: 6-, 12- and 15-month postoperative uncorrected- and best spectacle-corrected visual acuity, steep and flat keratometry, manifest sphere and astigmatism, rate of conversion to penetrating keratoplasty (PK), big-bubble success, central corneal thickness, endothelial cell count and complications.
Results: In intention-to-treat analysis, mean postoperative astigmatism in the FE-DALK (n = 30) and S-DALK (n = 30) groups at 15 months was 7.8 ± 4.4 D and 6.3 ± 5.0 D, respectively (p = 0.282) with an adjusted mean difference of 1.3 D (95% CI -1.08, +3.65). Mean SIA (arithmetic) was 9.2 ± 7.8 and 8.8 ± 5.4 D, respectively (p = 0.838) with a mean difference of 0.4 D (95% CI -3.13, +3.85). In an analysis of successful DALK cases only, mean postoperative astigmatism in the FE-DALK (n = 24) and S-DALK (n = 20) groups at 15 months (after excluding 4 eyes with AEs) was 7.3 ± 4.4 and 6.2 ± 4.9 D, respectively (p = 0.531) with an adjusted mean difference of 0.9 D (95% CI -1.94, +3.71). Mean SIA (arithmetic) was 9.1 ± 7.8 and 7.9 ± 4.6 D, respectively (p = 0.547) with a mean difference of 1.2 D (95% CI -2.70,+5.02). Comparison of secondary outcomes showed only weak statistical evidence.
Conclusions: In this randomized controlled trial, FE-DALK and S-DALK showed comparable functional and anatomical outcomes.
© 2023. The Author(s), under exclusive licence to The Royal College of Ophthalmologists.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Comparison of outcomes and complications of deep anterior lamellar keratoplasty and penetrating keratoplasty performed in a large group of patients with keratoconus.Int Ophthalmol. 2018 Jun;38(3):985-992. doi: 10.1007/s10792-017-0548-9. Epub 2017 May 22. Int Ophthalmol. 2018. PMID: 28534231
-
Comparative study of keratoconus between Anwar's deep anterior lamellar keratoplasty versus converted penetrating keratoplasty.Arch Soc Esp Oftalmol. 2015 Jun;90(6):257-63. doi: 10.1016/j.oftal.2014.11.008. Epub 2015 Mar 25. Arch Soc Esp Oftalmol. 2015. PMID: 25817955 English, Spanish.
-
Outcomes of deep anterior lamellar keratoplasty versus intralase enabled penetrating keratoplasty in keratoconus.Can J Ophthalmol. 2011 Oct;46(5):403-7. doi: 10.1016/j.jcjo.2011.07.003. Epub 2011 Aug 4. Can J Ophthalmol. 2011. PMID: 21995982
-
Systematic review comparing penetrating keratoplasty and deep anterior lamellar keratoplasty for management of keratoconus.Cont Lens Anterior Eye. 2017 Feb;40(1):3-14. doi: 10.1016/j.clae.2016.10.001. Epub 2016 Oct 29. Cont Lens Anterior Eye. 2017. PMID: 27802912
-
Comparison of Femtosecond Laser Assistance and Manual Trephination in Deep Anterior Lamellar Keratoplasty in the Treatment of Keratoconus: A Meta-Analysis.Am J Ophthalmol. 2023 Dec;256:126-137. doi: 10.1016/j.ajo.2023.08.003. Epub 2023 Aug 6. Am J Ophthalmol. 2023. PMID: 37553035
References
-
- Archila EA. Deep lamellar keratoplasty dissection of host tissue with intrastromal air injection. Cornea. 1984;3:217–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
