

Adherence to recommended physical activity restrictions due to threatened preterm delivery - a descriptive multi-center study
- PMID: 36694170
- PMCID: PMC9872354
- DOI: 10.1186/s12884-023-05371-5
Adherence to recommended physical activity restrictions due to threatened preterm delivery - a descriptive multi-center study
Abstract
Background: Threatened preterm delivery is a serious obstetrical complication and has for decades been prescribed physical activity restrictions (AR). Adherence to the recommended level of physical AR is however unknown. This study aimed to assess the objectively measured different physical positions and activities of pregnant women recommended AR due to threatened preterm delivery complications, compared to a reference group of uncomplicated pregnant women without restrictions, and to explore if admission status influenced adherence to AR.
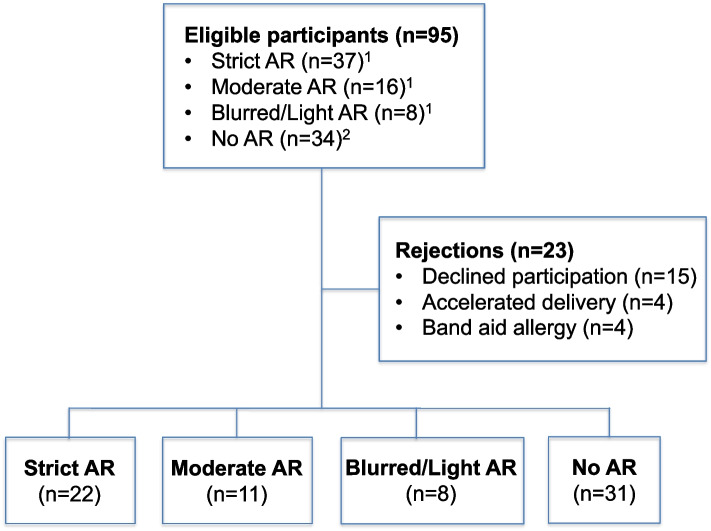
Methods: A Danish descriptive, clinical multi-center study included singleton pregnancies between 22-33 gestational weeks admitted to an antenatal ward or during midwife consultations either prescribed AR due to threatened preterm delivery or uncomplicated controls without restrictions. For seven days participants wore two tri-axial accelerometric SENS® monitors. Accelerometric data included time spent in five different positions, activities, and step counts. At inclusion demographic and obstetric information was collected.
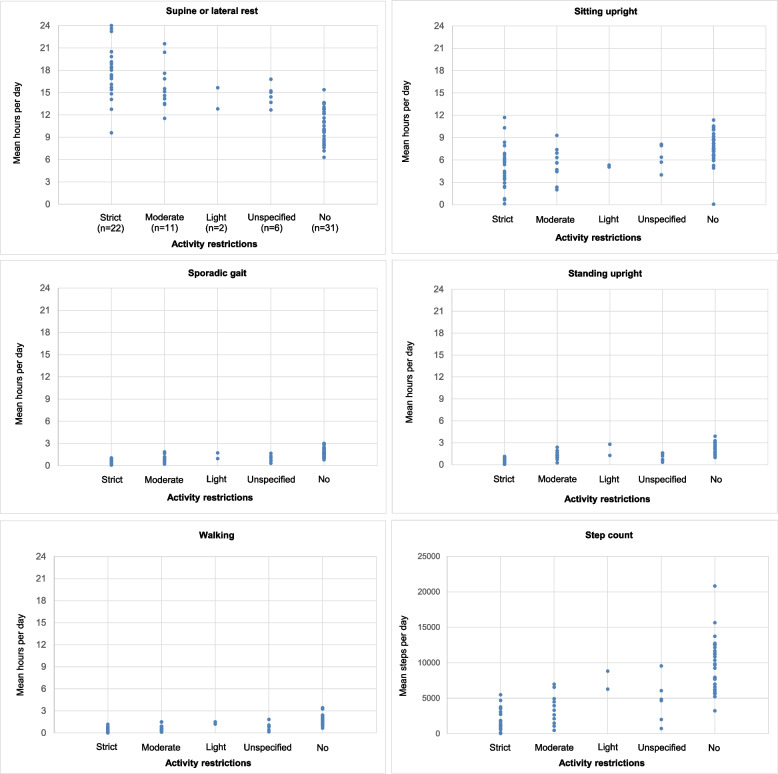
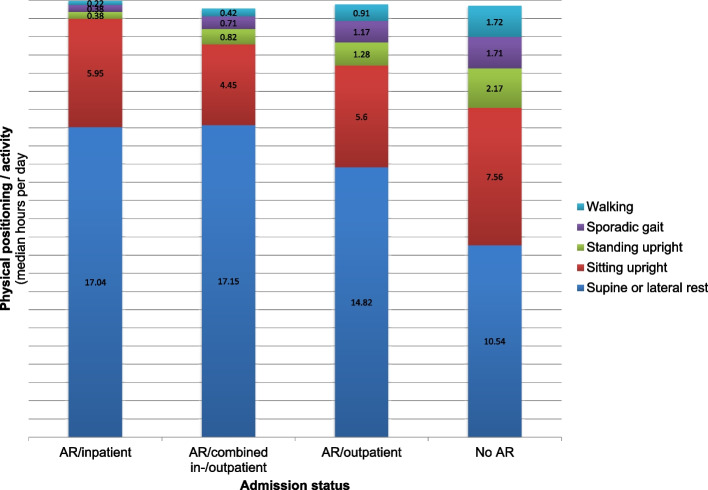
Results: Seventy-two pregnant women participated; 31% were prescribed strict AR, 15% moderate, 3% light, 8% unspecified, and 43% had no AR. Strict AR participants rested in the supine/lateral position for 17.7 median hours/day (range:9.6-24.0); sat upright 4.9 h/day (0.11-11.7); took 1,520steps/day (20-5,482), and 64% were inpatients. Moderate AR participants rested in the supine/lateral position for 15.1 h/day (11.5-21.6); sat upright 5.6 h/day (2.0-9.3); took 3,310steps/day (467-6,968), and 64% were outpatients. Participants with no AR rested 10.5 h/day (6.3-15.4) in supine/lateral position; sat upright 7.6 h/day (0.1-11.4) and took 9,235steps/day (3,225-20,818). Compared to no restrictions, participants with strict or moderate AR spent significant more time in physical resting positions and took significant fewer mean steps. Among strict AR admission status did not alter time spent in the physical positions, nor the step count.
Conclusions: Overall, participants adhered highly to the recommended AR. However, discriminating between strict and moderate AR recommendations did not alter how physical resting positions and activities were carried out. The admission status did not influence how participants adhered to strict AR.
Keywords: Accelerometric data; Activity restrictions; Adherence; Admission status; Physical positions/movements; Threatened preterm delivery.
© 2023. The Author(s).
Conflict of interest statement
All authors state explicitly that they have no conflicts of interest in relation to this article.
Figures
Similar articles
-
Quantitative activity levels and gestational age at delivery: a prospective cohort study among nulliparous women.Am J Obstet Gynecol MFM. 2022 Jan;4(1):100503. doi: 10.1016/j.ajogmf.2021.100503. Epub 2021 Oct 17. Am J Obstet Gynecol MFM. 2022. PMID: 34666197
-
The evaluation of maternal systemic thiol/disulphide homeostasis for the short-term prediction of preterm birth in women with threatened preterm labour: a pilot study.J Obstet Gynaecol. 2022 Aug;42(6):1972-1977. doi: 10.1080/01443615.2022.2056829. Epub 2022 Jun 1. J Obstet Gynaecol. 2022. PMID: 35648800
-
Effectiveness of a cervical pessary for women who did not deliver 48 h after threatened preterm labor (Assessment of perinatal outcome after specific treatment in early labor: Apostel VI trial).BMC Pregnancy Childbirth. 2016 Jul 12;16(1):154. doi: 10.1186/s12884-016-0935-7. BMC Pregnancy Childbirth. 2016. PMID: 27405353 Free PMC article. Clinical Trial.
-
Maternal position in the second stage of labour for women with epidural anaesthesia.Cochrane Database Syst Rev. 2018 Nov 9;11(11):CD008070. doi: 10.1002/14651858.CD008070.pub4. Cochrane Database Syst Rev. 2018. PMID: 30411804 Free PMC article.
-
[Prevention of spontaneous preterm birth (excluding preterm premature rupture of membranes): Guidelines for clinical practice - Text of the Guidelines (short text)].J Gynecol Obstet Biol Reprod (Paris). 2016 Dec;45(10):1446-1456. doi: 10.1016/j.jgyn.2016.09.011. Epub 2016 Nov 9. J Gynecol Obstet Biol Reprod (Paris). 2016. PMID: 27836377 Review. French.
Cited by
-
Monitoring postures and motions of hospitalized patients using sensor technology: a scoping review.Ann Med. 2024 Dec;56(1):2399963. doi: 10.1080/07853890.2024.2399963. Epub 2024 Sep 6. Ann Med. 2024. PMID: 39239877 Free PMC article.
References
-
- Bendix J. Activity restriction and hospitalisation in threatened preterm delivery. PhD Thesis. University of Copenhagen; 2015.
-
- Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, Narwal R, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379(9832):2162–2172. doi: 10.1016/S0140-6736(12)60820-4. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
