

Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association
- PMID: 36695182
- PMCID: PMC12135016
- DOI: 10.1161/CIR.0000000000001123
Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association
Erratum in
-
Correction to: Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association.Circulation. 2023 Feb 21;147(8):e622. doi: 10.1161/CIR.0000000000001137. Epub 2023 Feb 20. Circulation. 2023. PMID: 36802886 No abstract available.
-
Correction to: Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association.Circulation. 2023 Jul 25;148(4):e4. doi: 10.1161/CIR.0000000000001167. Epub 2023 Jul 24. Circulation. 2023. PMID: 37486999 No abstract available.
Abstract
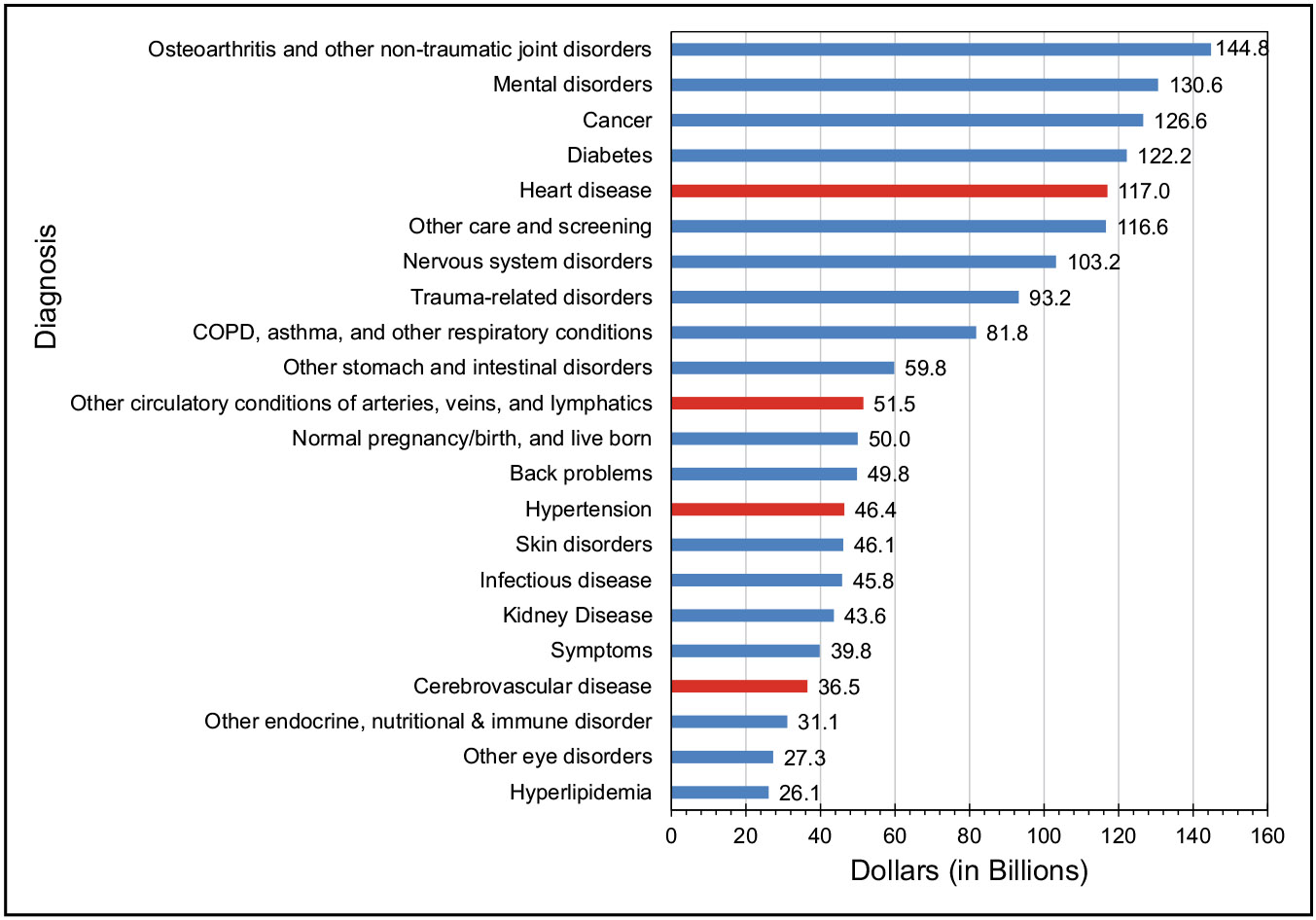
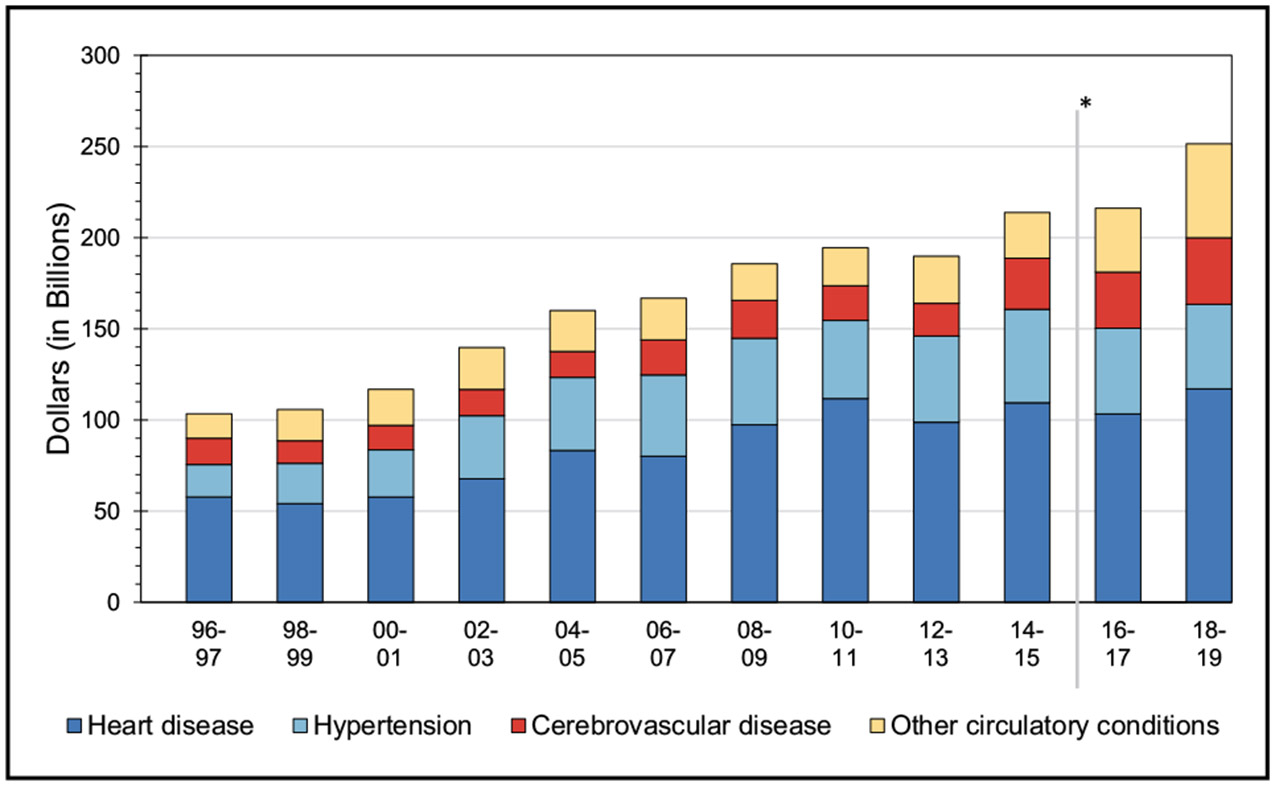
Background: The American Heart Association, in conjunction with the National Institutes of Health, annually reports the most up-to-date statistics related to heart disease, stroke, and cardiovascular risk factors, including core health behaviors (smoking, physical activity, diet, and weight) and health factors (cholesterol, blood pressure, and glucose control) that contribute to cardiovascular health. The Statistical Update presents the latest data on a range of major clinical heart and circulatory disease conditions (including stroke, congenital heart disease, rhythm disorders, subclinical atherosclerosis, coronary heart disease, heart failure, valvular disease, venous disease, and peripheral artery disease) and the associated outcomes (including quality of care, procedures, and economic costs).
Methods: The American Heart Association, through its Epidemiology and Prevention Statistics Committee, continuously monitors and evaluates sources of data on heart disease and stroke in the United States to provide the most current information available in the annual Statistical Update with review of published literature through the year before writing. The 2023 Statistical Update is the product of a full year's worth of effort in 2022 by dedicated volunteer clinicians and scientists, committed government professionals, and American Heart Association staff members. The American Heart Association strives to further understand and help heal health problems inflicted by structural racism, a public health crisis that can significantly damage physical and mental health and perpetuate disparities in access to health care, education, income, housing, and several other factors vital to healthy lives. This year's edition includes additional COVID-19 (coronavirus disease 2019) publications, as well as data on the monitoring and benefits of cardiovascular health in the population, with an enhanced focus on health equity across several key domains.
Results: Each of the chapters in the Statistical Update focuses on a different topic related to heart disease and stroke statistics.
Conclusions: The Statistical Update represents a critical resource for the lay public, policymakers, media professionals, clinicians, health care administrators, researchers, health advocates, and others seeking the best available data on these factors and conditions.
Keywords: AHA Scientific Statements; cardiovascular diseases; epidemiology; risk factors; statistics; stroke.
Conflict of interest statement
The American Heart Association makes every effort to avoid any actual or potential conflicts of interest that may arise as a result of an outside relationship or a personal, professional, or business interest of a member of the writing panel. Specifically, all members of the writing group are required to complete and submit a Disclosure Questionnaire showing all such relationships that might be perceived as real or potential conflicts of interest.
Figures



























































References
-
- Lloyd-Jones DM, Allen NB, Anderson CAM, Black T, Brewer LC, Foraker RE, Grandner MA, Lavretsky H, Perak AM, Sharma G, et al. ; on behalf of the American Heart Association. Life’s Essential 8: updating and enhancing the American Heart Association’s construct of cardiovascular health: a presidential advisory from the American Heart Association. Circulation. 2022;146:e18–e43. doi: 10.1161/CIR.0000000000001078 - DOI - PMC - PubMed
-
- Centers for Disease Control and Prevention and National Center for Health Statistics. National Vital Statistics System: public use data file documentation: mortality multiple cause-of-death micro-data files. Accessed April 8, 2022. https://www.cdc.gov/nchs/nvss/mortality_public_use_data.htm
-
- Centers for Disease Control and Prevention and National Center for Health Statistics. Multiple cause of death, CDC WONDER online database. Accessed April 1, 2022. https://wonder.cdc.gov/mcd-icd10.html
-
- US Census Bureau. US Census Bureau population estimates: historical data: 2000. Accessed April 1, 2022. https://www.census.gov/programs-surveys/popest.html
-
- Anderson RN, Minino AM, Hoyert DL, Rosenberg HM. Comparability of cause of death between ICD-9 and ICD-10: preliminary estimates. Natl Vital Stat Rep. 2001;49:1–32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
