

Mechanical Dyssynchrony of Isolated Left and Right Ventricular Human Myocardium in End-Stage Heart Failure
- PMID: 36695183
- PMCID: PMC10033321
- DOI: 10.1161/CIRCHEARTFAILURE.122.009871
Mechanical Dyssynchrony of Isolated Left and Right Ventricular Human Myocardium in End-Stage Heart Failure
Abstract
Background: The left and right ventricles of the human heart differ in embryology, shape, thickness, and function. Ventricular dyssynchrony often occurs in cases of heart failure. Our objectives were to assess whether differences in contractile properties exist between the left and right ventricles and to evaluate signs of left/right ventricular mechanical synchrony in isolated healthy and diseased human myocardium.
Methods: Myocardial left and right ventricular trabeculae were dissected from nonfailing and end-stage failing human hearts. Baseline contractile force and contraction/relaxation kinetics of the left ventricle were compared to those of the right ventricle in the nonfailing group (n=41) and in the failing group (n=29). Correlation analysis was performed to assess the mechanical synchrony between left and right ventricular myocardium isolated from the same heart, in nonfailing (n=41) and failing hearts (n=29).
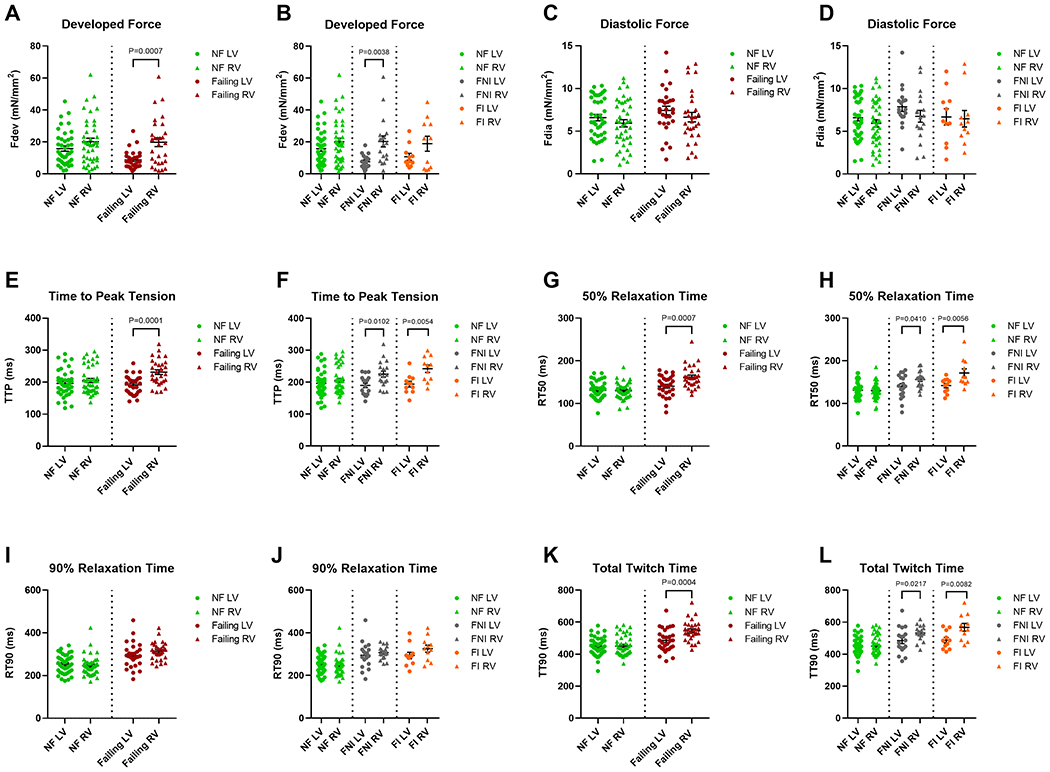
Results: The failing right ventricular myocardium showed significantly higher developed force (Fdev; P=0.001; d=0.98), prolonged time to peak (P<0.001; d=1.14), and higher rate of force development (P=0.002; d=0.89) and force decline (P=0.003; d=0.82) compared to corresponding left ventricular myocardium. In healthy myocardium, a strong positive relationship was present between the left and right ventricles in time to peak (r=0.58, P<0.001) and maximal kinetic rate of contraction (r=0.63, P<0.001). These coefficients were much weaker, often nearly absent, in failing myocardium.
Conclusions: At the level of isolated cardiac trabeculae, contractile performance, specifically of contractile kinetics, is correlated in the nonfailing myocardium between the left and right ventricles' but this correlation is significantly weaker, or even absent, in end-stage heart failure, suggesting an interventricular mechanical dyssynchrony.
Keywords: contractility; heart failure; left ventricle; mechanical dyssynchrony; myocardium; right ventricle.
Conflict of interest statement
Disclosures
Dr Nahush Mokadam serves as a consultant for Abbott, Medtronic, SynCardia and Xylocor and on the Clinical Events Committee for Carmat. The other authors have no conflicts of interest, financial or otherwise to declare.
Figures





References
-
- Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, Boehme AK, Buxton AE, Carson AP, Commodore-Mensah Y, et al. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation. 2022;145:e153–e639. - PubMed
-
- Rodriguez LM, Timmermans C, Nabar A, Beatty G, Wellens HJ. Variable patterns of septal activation in patients with left bundle branch block and heart failure. Journal of Cardiovascular Electrophysiology. 2003;14:135–141. - PubMed
-
- Kashani A, Barold SS. Significance of QRS complex duration in patients with heart failure. Journal of the American College of Cardiology. 2005;46:2183–2192. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
