

Phenotyping of Elderly Patients With Heart Failure Focused on Noncardiac Conditions: A Latent Class Analysis From a Multicenter Registry of Patients Hospitalized With Heart Failure
- PMID: 36695300
- PMCID: PMC9973643
- DOI: 10.1161/JAHA.122.027689
Phenotyping of Elderly Patients With Heart Failure Focused on Noncardiac Conditions: A Latent Class Analysis From a Multicenter Registry of Patients Hospitalized With Heart Failure
Abstract
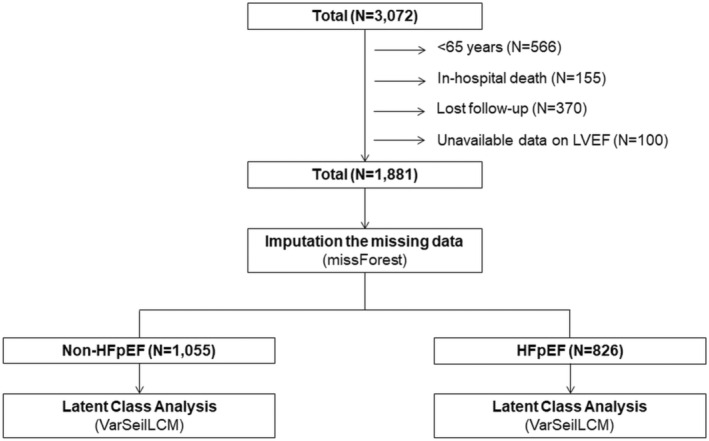
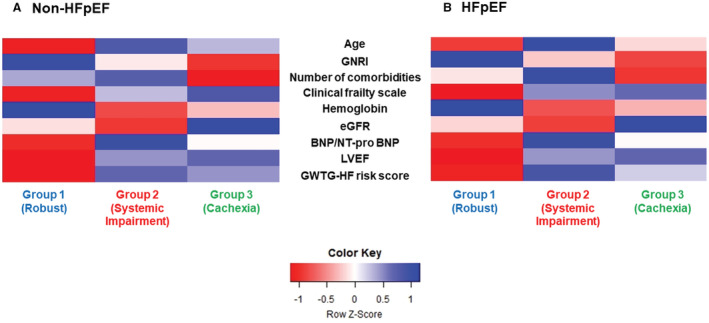
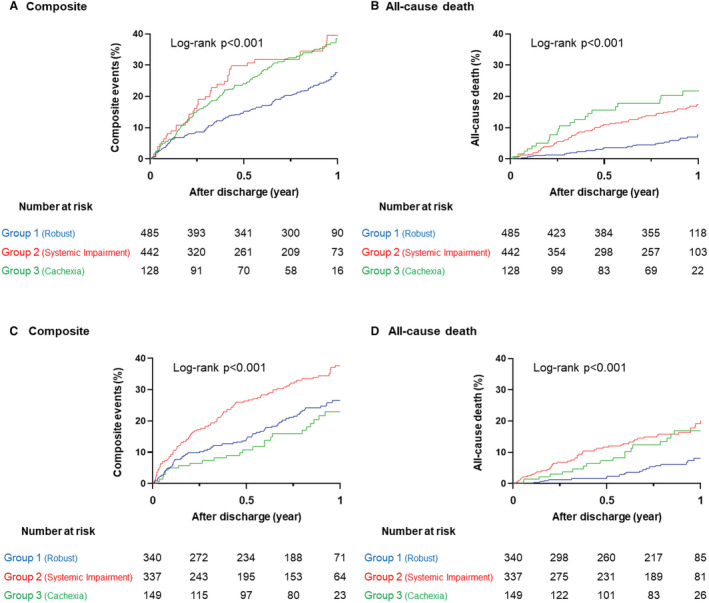
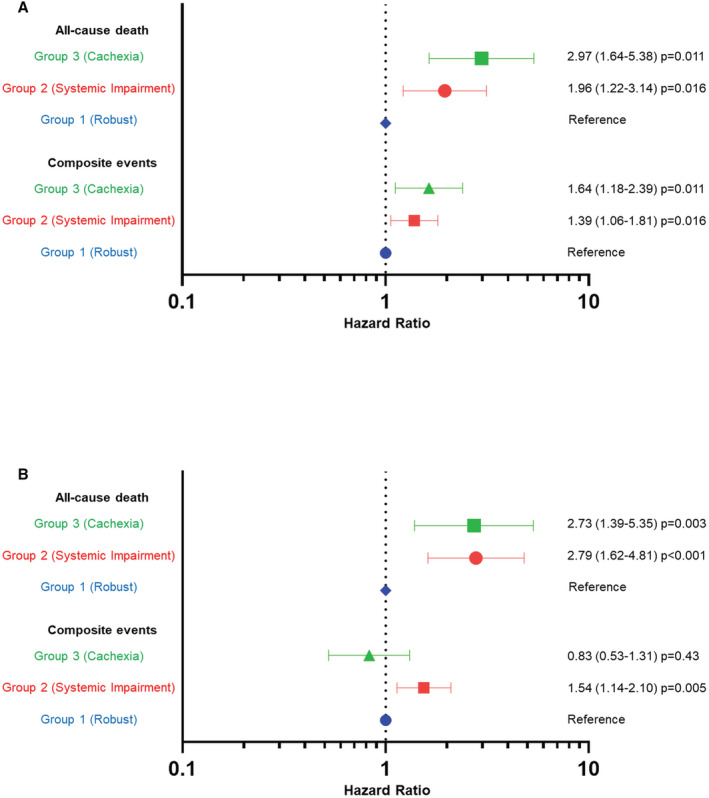
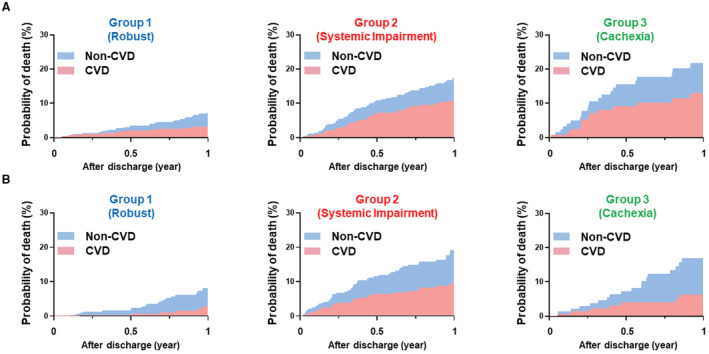
Background The burden of noncardiovascular conditions is becoming increasingly prevalent in patients with heart failure (HF). We aimed to identify novel phenogroups incorporating noncardiovascular conditions to facilitate understanding and risk stratification in elderly patients with HF. Methods and Results Data from a total of 1881 (61.2%) patients aged ≥65 years were extracted from a prospective multicenter registry of patients hospitalized for acute HF (N=3072). We constructed subgroups of patients with HF with preserved ejection fraction (HFpEF; N=826, 43.9%) and those with non-HFpEF (N=1055, 56.1%). Latent class analysis was performed in each subgroup using 17 variables focused on noncardiovascular conditions (including comorbidities, Clinical Frailty Scale, and Geriatric Nutritional Risk Index). The latent class analysis revealed 3 distinct clinical phenogroups in both HFpEF and non-HFpEF subgroups: (1) robust physical and nutritional status (Group 1: HFpEF, 41.2%; non-HFpEF, 46.0%); (2) multimorbid patients with renal impairment (Group 2: HFpEF, 40.8%; non-HFpEF, 41.9%); and (3) malnourished patients (Group 3: HFpEF, 18.0%; non-HFpEF, 12.1%). After multivariable adjustment, compared with Group 1, patients in Groups 2 and 3 had a higher risk for all-cause death over the 1-year postdischarge period (hazard ratio [HR], 2.79 [95% CI, 1.64-4.81] and HR, 2.73 [95% CI, 1.39-5.35] in HFpEF; HR, 1.96 [95% CI, 1.22-3.14] and HR, 2.97 [95% CI, 1.64-5.38] in non-HFpEF; respectively). Conclusions In elderly patients with HF, the phenomapping focused on incorporating noncardiovascular conditions identified 3 phenogroups, each representing distinct clinical outcomes, and the discrimination pattern was similar for both patients with HFpEF and non-HFpEF. This classification provides novel risk stratification and may aid in clinical decision making.
Keywords: elderly patients; heart failure; noncardiovascular conditions; phenotyping.
Figures
Similar articles
-
Distinct implications of body mass index in different subgroups of nonobese patients with heart failure with preserved ejection fraction: a latent class analysis of data from the TOPCAT trial.BMC Med. 2022 Nov 2;20(1):423. doi: 10.1186/s12916-022-02626-4. BMC Med. 2022. PMID: 36324141 Free PMC article. Clinical Trial.
-
Comprehensive characterization of non-cardiac comorbidities in acute heart failure: an analysis of ESC-HFA EURObservational Research Programme Heart Failure Long-Term Registry.Eur J Prev Cardiol. 2023 Sep 20;30(13):1346-1358. doi: 10.1093/eurjpc/zwad151. Eur J Prev Cardiol. 2023. PMID: 37172316
-
Clinical Phenogroups in Heart Failure With Preserved Ejection Fraction: Detailed Phenotypes, Prognosis, and Response to Spironolactone.JACC Heart Fail. 2020 Mar;8(3):172-184. doi: 10.1016/j.jchf.2019.09.009. Epub 2020 Jan 8. JACC Heart Fail. 2020. PMID: 31926856 Free PMC article. Clinical Trial.
-
Heart failure with preserved ejection fraction phenogroup classification using machine learning.ESC Heart Fail. 2023 Jun;10(3):2019-2030. doi: 10.1002/ehf2.14368. Epub 2023 Apr 12. ESC Heart Fail. 2023. PMID: 37051638 Free PMC article.
-
Causes and Temporal Patterns of 30-Day Readmission Among Older Adults Hospitalized With Heart Failure With Preserved or Reduced Ejection Fraction.J Am Heart Assoc. 2018 Apr 23;7(9):e007785. doi: 10.1161/JAHA.117.007785. J Am Heart Assoc. 2018. PMID: 29686028 Free PMC article.
Cited by
-
Association of Tricuspid Regurgitation With Mortality in Heart Failure With Left-Sided Heart Disease.JACC Adv. 2025 Jun;4(6 Pt 1):101832. doi: 10.1016/j.jacadv.2025.101832. Epub 2025 May 26. JACC Adv. 2025. PMID: 40424674 Free PMC article.
-
Demographics and Clinical Characteristics among Patients with Distinct Psychosocial Burden Profiles Related to Vitiligo: Results of a Latent Class Analysis.Dermatol Ther (Heidelb). 2025 May;15(5):1195-1208. doi: 10.1007/s13555-025-01401-6. Epub 2025 Apr 10. Dermatol Ther (Heidelb). 2025. PMID: 40208558 Free PMC article.
-
Phenotypic Trajectories From Acute to Stable Phase in Heart Failure With Preserved Ejection Fraction: Insights From the PURSUIT-HFpEF Study.J Am Heart Assoc. 2025 Feb 4;14(3):e037567. doi: 10.1161/JAHA.124.037567. Epub 2025 Feb 3. J Am Heart Assoc. 2025. PMID: 39895530 Free PMC article.
-
Temporal Trends in Heart Failure Management and Outcomes: Insights From a Japanese Multicenter Registry of Tertiary Care Centers.J Am Heart Assoc. 2023 Nov 7;12(21):e031179. doi: 10.1161/JAHA.123.031179. Epub 2023 Nov 6. J Am Heart Assoc. 2023. PMID: 37929712 Free PMC article.
-
Sex-specific cardiometabolic multimorbidity, metabolic syndrome and left ventricular function in heart failure with preserved ejection fraction in the UK Biobank.Cardiovasc Diabetol. 2025 Jun 4;24(1):238. doi: 10.1186/s12933-025-02788-4. Cardiovasc Diabetol. 2025. PMID: 40468351 Free PMC article.
References
-
- Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Cheng S, Delling FN, et al. Heart disease and stroke statistics‐2021 update: a report from the American Heart Association. Circulation. 2021;143:e254–e743. doi: 10.1161/CIR.0000000000000950 - DOI - PubMed
-
- Abbafati C, Abbas KM, Abbasi‐Kangevari M, Abd‐Allah F, Abdelalim A, Abdollahi M, Abdollahpour I, Abegaz KH, Abolhassani H, Aboyans V, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396:1204–1222. doi: 10.1016/S0140-6736(20)30925-9 - DOI - PMC - PubMed
-
- Ueda T, Kawakami R, Horii M, Sugawara Y, Matsumoto T, Okada S, Nishida T, Soeda T, Okayama S, Somekawa S, et al. Noncardiovascular death, especially infection, is a significant cause of death in elderly patients with acutely decompensated heart failure. J Card Fail. 2014;20:174–180. doi: 10.1016/j.cardfail.2013.12.007 - DOI - PubMed
-
- Tromp J, Shen L, Jhund PS, Anand IS, Carson PE, Desai AS, Granger CB, Komajda M, McKelvie RS, Pfeffer MA, et al. Age‐related characteristics and outcomes of patients with heart failure with preserved ejection fraction. J Am Coll Cardiol. 2019;74:601–612. doi: 10.1016/j.jacc.2019.05.052 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
