

Prenatal Exposure to Oxidative Potential and Lung Function in Infants and Preschool- Age Children: A Prospective Study
- PMID: 36695591
- PMCID: PMC9875724
- DOI: 10.1289/EHP11155
Prenatal Exposure to Oxidative Potential and Lung Function in Infants and Preschool- Age Children: A Prospective Study
Abstract
Background: Fine particulate matter () has been found to be detrimental to respiratory health of children, but few studies have examined the effects of prenatal oxidative potential (OP) on lung function in infants and preschool children.
Objectives: We estimated the associations of personal exposure to and OP during pregnancy on offspring objective lung function parameters and compared the strengths of associations between both exposure metrics.
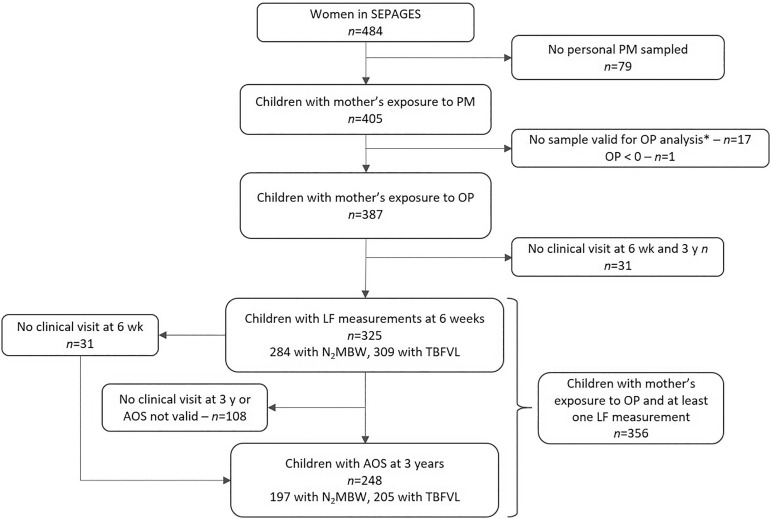
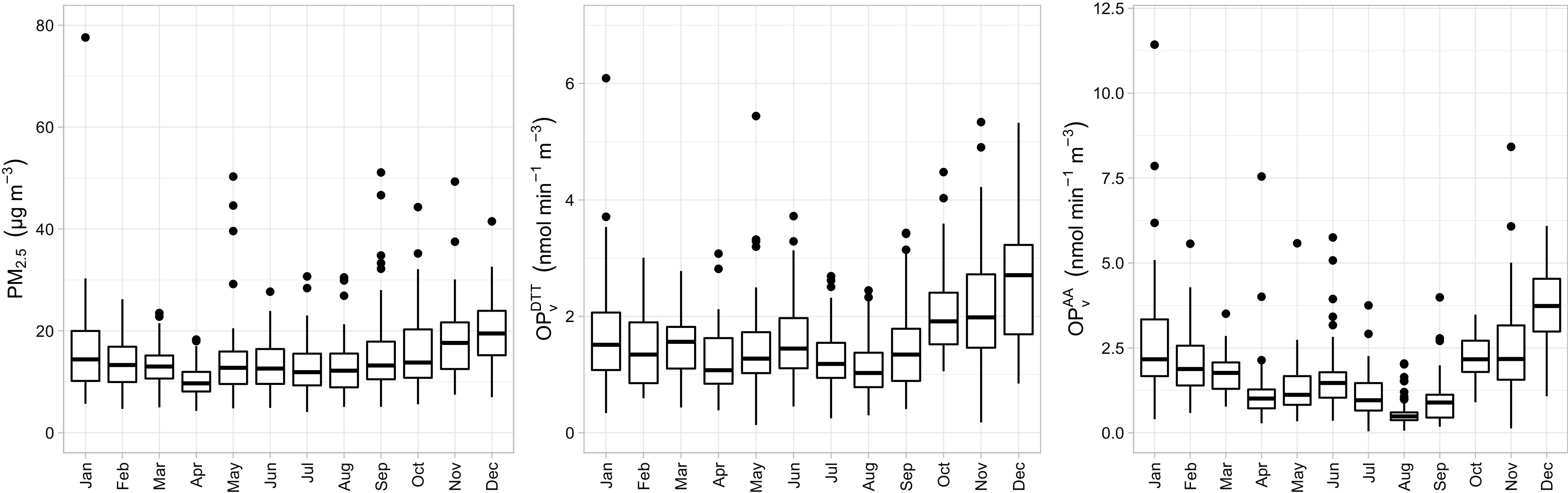
Methods: We used data from 356 mother-child pairs from the SEPAGES cohort. PM filters collected twice during a week were analyzed for OP, using the dithiothreitol (DTT) and the ascorbic acid (AA) assays, quantifying the exposure of each pregnant woman. Lung function was assessed with tidal breathing analysis (TBFVL) and nitrogen multiple-breath washout () test, performed at 6 wk, and airwave oscillometry (AOS) performed at 3 y. Associations of prenatal mass and OP with lung function parameters were estimated using multiple linear regressions.
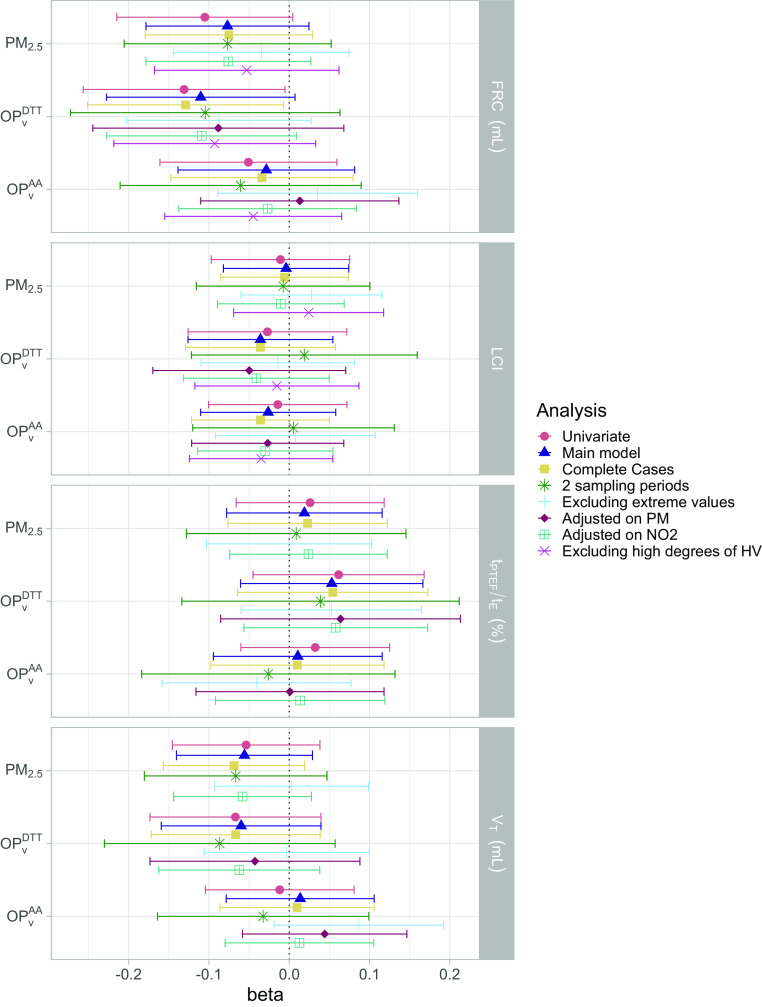
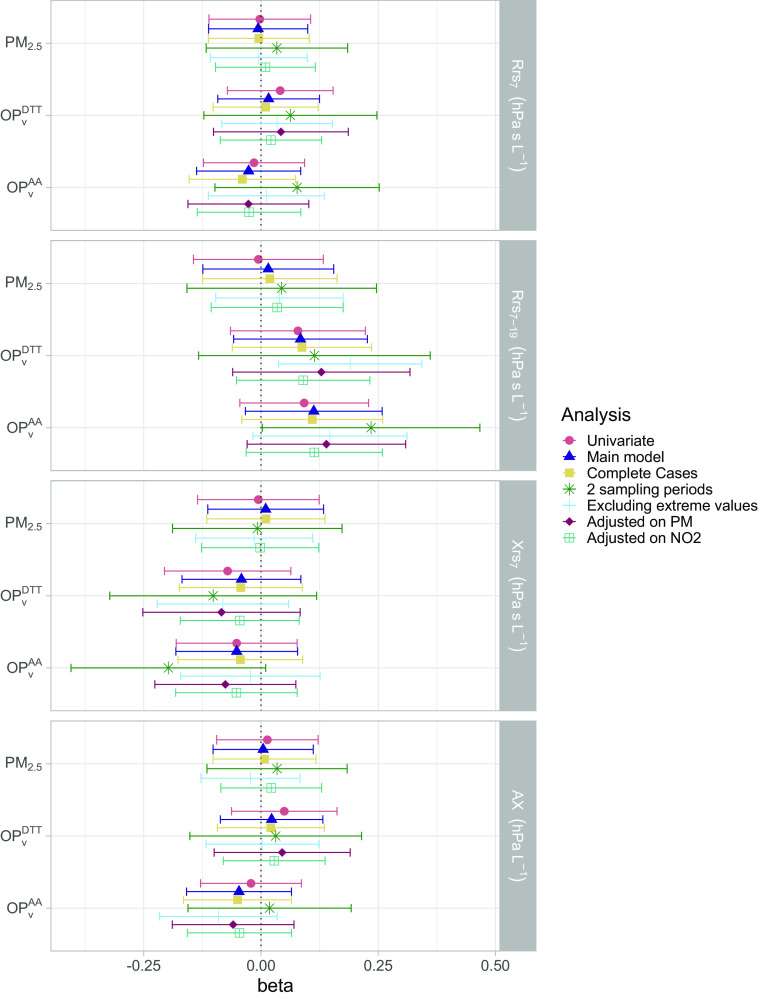
Results: In neonates, an interquartile (IQR) increase in () was associated with a decrease in functional residual capacity (FRC) measured by [; 95% confidence interval (CI): , 0.15]. Associations with showed similar patterns in comparison with but of smaller magnitude. Lung clearance index (LCI) and TBFVL parameters did not show any clear association with the exposures considered. At 3 y, increased frequency-dependent resistance of the lungs () from AOS tended to be associated with higher (; 95% CI: , 0.24) and (; ; 95% CI: , 0.27) but not with (; ; 95% CI: , 0.16). Results for FRC and remained similar in OP models adjusted on .
Discussion: Prenatal exposure to was associated with several offspring lung function parameters over time, all related to lung volumes. https://doi.org/10.1289/EHP11155.
Figures
Similar articles
-
Pre-natal exposure to NO2 and PM2.5 and newborn lung function: An approach based on repeated personal exposure measurements.Environ Res. 2023 Jun 1;226:115656. doi: 10.1016/j.envres.2023.115656. Epub 2023 Mar 10. Environ Res. 2023. PMID: 36906269
-
Prenatal Exposure to Air Pollution and Respiratory Distress in Term Newborns: Results from the MIREC Prospective Pregnancy Cohort.Environ Health Perspect. 2024 Jan;132(1):17007. doi: 10.1289/EHP12880. Epub 2024 Jan 25. Environ Health Perspect. 2024. PMID: 38271058 Free PMC article.
-
Effects of personal exposure to the oxidative potential of PM2.5 on oxidative stress biomarkers in pregnant women.Sci Total Environ. 2024 Feb 10;911:168475. doi: 10.1016/j.scitotenv.2023.168475. Epub 2023 Nov 10. Sci Total Environ. 2024. PMID: 37951259
-
Association between prenatal exposure to ambient particulate matter and risk of hypospadias in offspring: A systematic review and meta-analysis.Environ Res. 2021 Jan;192:110190. doi: 10.1016/j.envres.2020.110190. Epub 2020 Sep 11. Environ Res. 2021. PMID: 32919959
-
Air pollution and children's health-a review of adverse effects associated with prenatal exposure from fine to ultrafine particulate matter.Environ Health Prev Med. 2021 Jul 12;26(1):72. doi: 10.1186/s12199-021-00995-5. Environ Health Prev Med. 2021. PMID: 34253165 Free PMC article. Review.
Cited by
-
Personal exposure to air pollutants and immune system biomarkers in pregnant women.Sci Rep. 2025 May 21;15(1):17672. doi: 10.1038/s41598-025-98712-7. Sci Rep. 2025. PMID: 40399383 Free PMC article.
-
Association between air pollutants and blood cell counts in pediatric patients with asthma: a retrospective observational study.BMC Public Health. 2025 Jan 24;25(1):306. doi: 10.1186/s12889-025-21517-w. BMC Public Health. 2025. PMID: 39856641 Free PMC article.
References
-
- Janssen NAH, Brunekreef B, van Vliet P, Aarts F, Meliefste K, Harssema H, et al. . 2003. The relationship between air pollution from heavy traffic and allergic sensitization, bronchial hyperresponsiveness, and respiratory symptoms in Dutch schoolchildren. Environ Health Perspect 111(12):1512–1518, PMID: , 10.1289/ehp.6243. - DOI - PMC - PubMed
-
- Murray CJL, Aravkin AY, Zheng P, Abbafati C, Abbas KM, Abbasi-Kangevari M, et al. . 2020. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet 396(10258):1223–1249, 10.1016/S0140-6736(20)30752-2. - DOI - PMC - PubMed
-
- WHO (World Health Organization). 2016. Ambient Air Pollution: A Global Assessment of Exposure and Burden of Disease. https://www.who.int/phe/publications/air-pollution-global-assessment/en/ [accessed 5 May 2021].
-
- Capello F, Pili G. 2018. Air Pollution in Infancy, Childhood and Young Adults. In: Clinical Handbook of Air Pollution-Related Diseases. Capello F, Gaddi AV, eds. Cham, Switzerland: Springer International Publishing, 141–186, 10.1007/978-3-319-62731-1_10. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
