

CD16+ natural killer cells in bronchoalveolar lavage are associated with antibody-mediated rejection and chronic lung allograft dysfunction
- PMID: 36695619
- PMCID: PMC10018437
- DOI: 10.1016/j.ajt.2022.10.006
CD16+ natural killer cells in bronchoalveolar lavage are associated with antibody-mediated rejection and chronic lung allograft dysfunction
Abstract
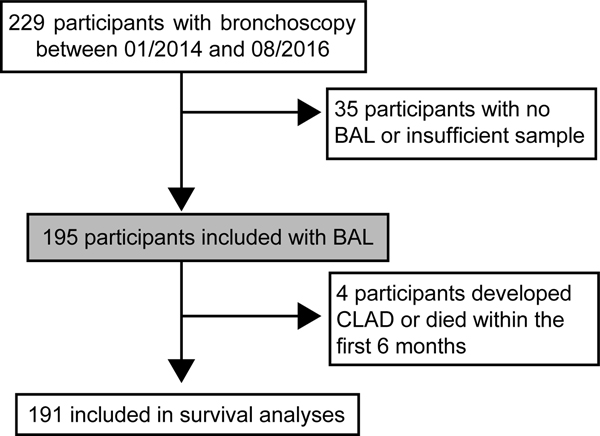
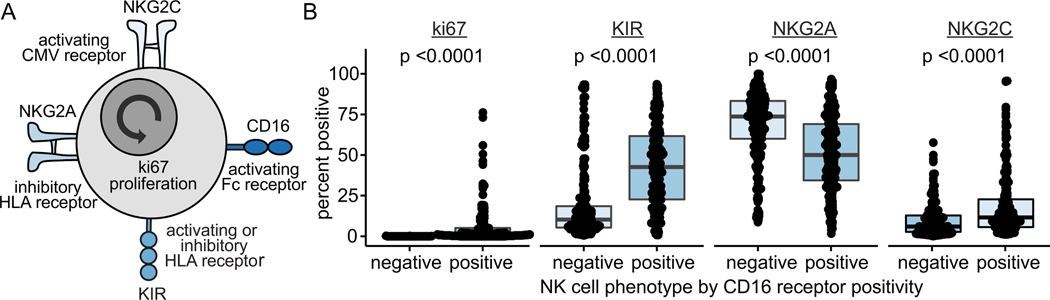
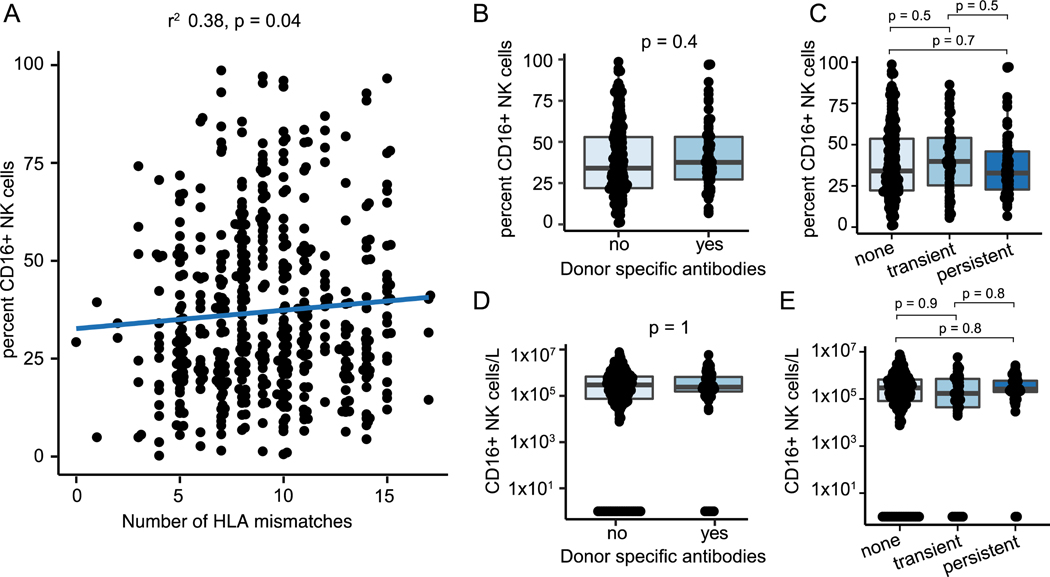
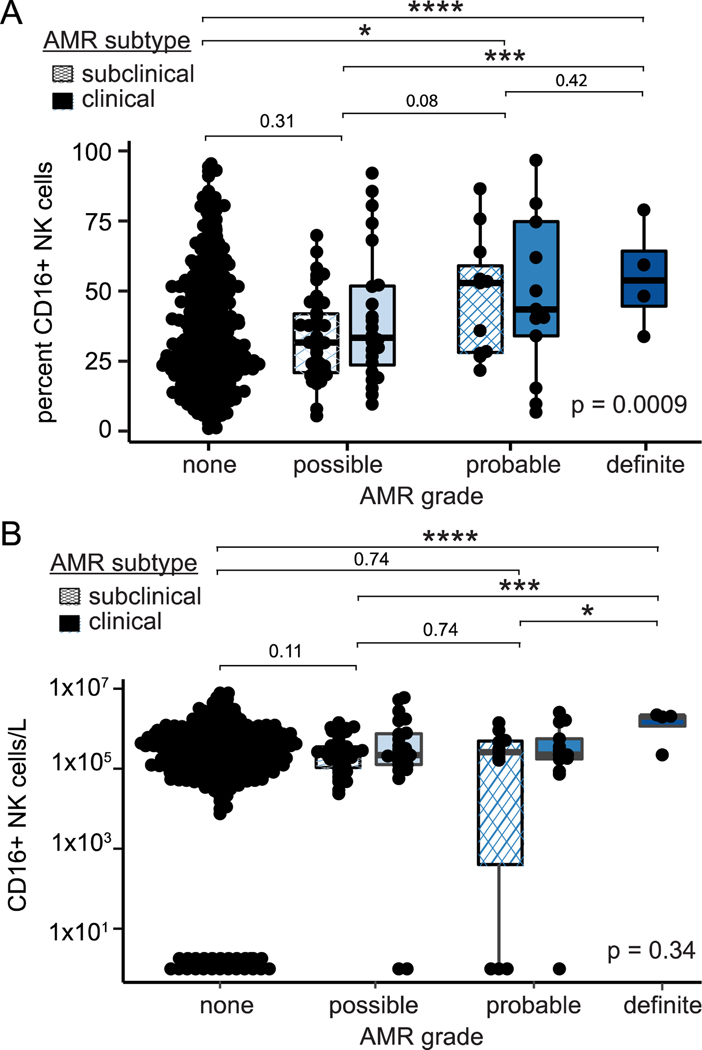
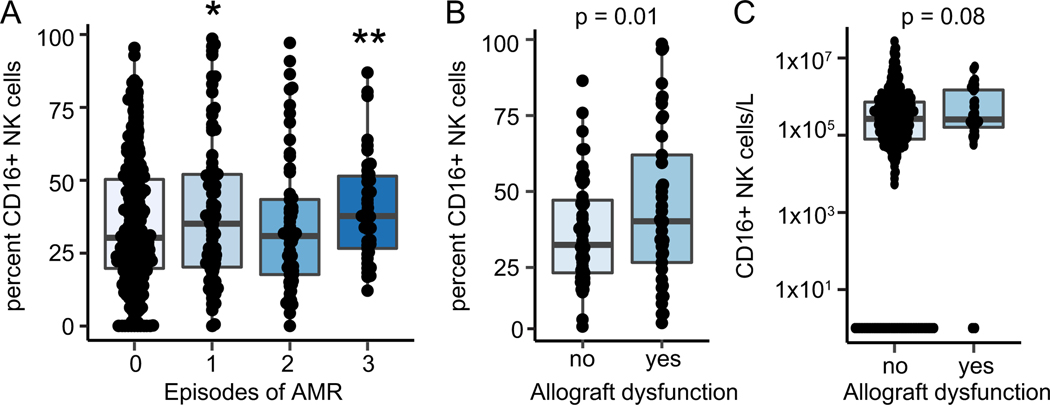
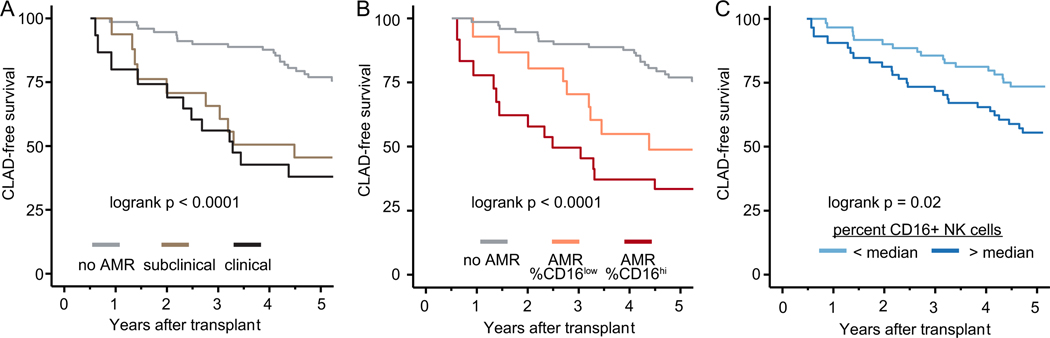
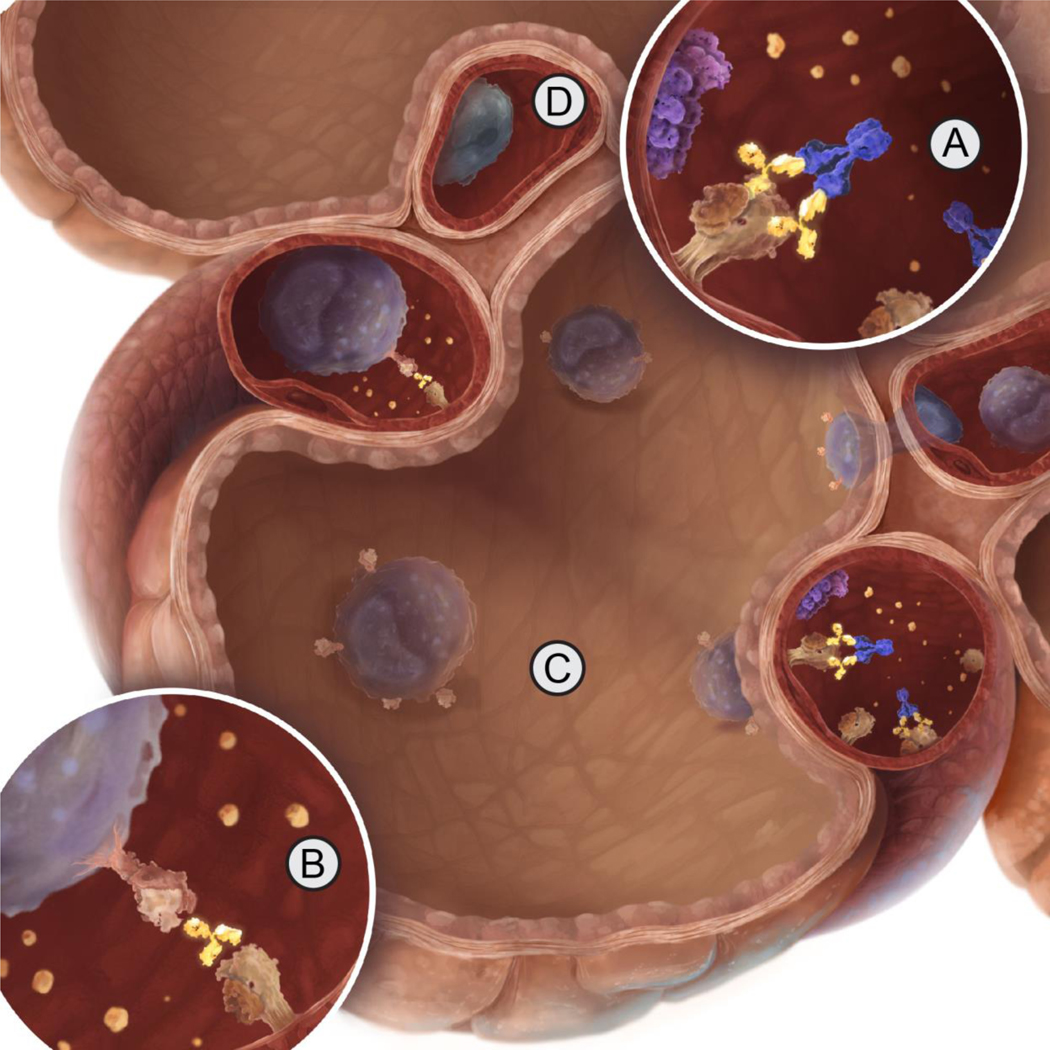
Acute and chronic rejections limit the long-term survival after lung transplant. Pulmonary antibody-mediated rejection (AMR) is an incompletely understood driver of long-term outcomes characterized by donor-specific antibodies (DSAs), innate immune infiltration, and evidence of complement activation. Natural killer (NK) cells may recognize DSAs via the CD16 receptor, but this complement-independent mechanism of injury has not been explored in pulmonary AMR. CD16+ NK cells were quantified in 508 prospectively collected bronchoalveolar lavage fluid samples from 195 lung transplant recipients. Associations between CD16+ NK cells and human leukocyte antigen mismatches, DSAs, and AMR grade were assessed by linear models adjusted for participant characteristics and repeat measures. Cox proportional hazards models were used to assess CD16+ NK cell association with chronic lung allograft dysfunction and survival. Bronchoalveolar lavage fluid CD16+ NK cell frequency was associated with increasing human leukocyte antigens mismatches and increased AMR grade. Although NK frequencies were similar between DSA+ and DSA- recipients, CD16+ NK cell frequencies were greater in recipients with AMR and those with concomitant allograft dysfunction. CD16+ NK cells were associated with long-term graft dysfunction after AMR and decreased chronic lung allograft dysfunction-free survival. These data support the role of CD16+ NK cells in pulmonary AMR.
Keywords: acute lung injury; biomarker; inflammation; innate immunity.
Published by Elsevier Inc.
Figures
Similar articles
-
FCGR3A and FCGR2A Genotypes Differentially Impact Allograft Rejection and Patients' Survival After Lung Transplant.Front Immunol. 2019 Jun 12;10:1208. doi: 10.3389/fimmu.2019.01208. eCollection 2019. Front Immunol. 2019. PMID: 31249568 Free PMC article.
-
Missing Self-Induced Activation of NK Cells Combines with Non-Complement-Fixing Donor-Specific Antibodies to Accelerate Kidney Transplant Loss in Chronic Antibody-Mediated Rejection.J Am Soc Nephrol. 2021 Feb;32(2):479-494. doi: 10.1681/ASN.2020040433. Epub 2020 Nov 25. J Am Soc Nephrol. 2021. PMID: 33239394 Free PMC article.
-
Interleukin-21 promotes Type-1 activation and cytotoxicity of CD56dimCD16bright natural killer cells during kidney allograft antibody-mediated rejection showing a new link between adaptive and innate humoral allo-immunity.Kidney Int. 2023 Oct;104(4):707-723. doi: 10.1016/j.kint.2023.04.024. Epub 2023 May 21. Kidney Int. 2023. PMID: 37220805 Free PMC article.
-
Natural Killer Cells: Critical Effectors During Antibody-mediated Rejection of Solid Organ Allografts.Transplantation. 2021 Feb 1;105(2):284-290. doi: 10.1097/TP.0000000000003298. Transplantation. 2021. PMID: 32384380 Review.
-
Interplay between immune responses to HLA and non-HLA self-antigens in allograft rejection.Hum Immunol. 2013 Nov;74(11):1478-85. doi: 10.1016/j.humimm.2013.07.002. Epub 2013 Jul 19. Hum Immunol. 2013. PMID: 23876679 Free PMC article. Review.
Cited by
-
The Transplant Bellwether: Endothelial Cells in Antibody-Mediated Rejection.J Immunol. 2023 Nov 1;211(9):1276-1285. doi: 10.4049/jimmunol.2300363. J Immunol. 2023. PMID: 37844279 Free PMC article. Review.
-
Circulating donor-derived cell-free DNA as a marker for rejection after lung transplantation.Front Immunol. 2023 Oct 11;14:1263389. doi: 10.3389/fimmu.2023.1263389. eCollection 2023. Front Immunol. 2023. PMID: 37885888 Free PMC article.
-
Macrophage and CD8 T cell discordance are associated with acute lung allograft dysfunction progression.J Heart Lung Transplant. 2024 Jul;43(7):1074-1086. doi: 10.1016/j.healun.2024.02.007. Epub 2024 Feb 15. J Heart Lung Transplant. 2024. PMID: 38367738 Free PMC article.
-
Immune dysregulation as a driver of bronchiolitis obliterans.Front Immunol. 2024 Dec 17;15:1455009. doi: 10.3389/fimmu.2024.1455009. eCollection 2024. Front Immunol. 2024. PMID: 39742269 Free PMC article. Review.
-
Prognostic significance and gene co-expression network of CD16A and FGL2 in gliomas.Front Oncol. 2024 Nov 19;14:1447113. doi: 10.3389/fonc.2024.1447113. eCollection 2024. Front Oncol. 2024. PMID: 39629005 Free PMC article.
References
-
- Meyer KC, Raghu G, Verleden GM et al. An international ISHLT/ATS/ERS clinical practice guideline: diagnosis and management of bronchiolitis obliterans syndrome. Eur Respir J 2014;44(6):1479–1503. - PubMed
-
- Le Pavec J, Suberbielle C, Lamrani L et al. De-novo donor-specific anti-HLA antibodies 30 days after lung transplantation are associated with a worse outcome. J Heart Lung Transplant 2016;35(9):1067–1077. - PubMed
-
- Angaswamy N, Saini D, Ramachandran S et al. Development of antibodies to human leukocyte antigen precedes development of antibodies to major histocompatibility class I-related chain A and are significantly associated with development of chronic rejection after human lung transplantation. Hum Immunol 2010;71(6):560–565. - PMC - PubMed
