

Immune Mechanisms in Epileptogenesis: Update on Diagnosis and Treatment of Autoimmune Epilepsy Syndromes
- PMID: 36696027
- PMCID: PMC9875200
- DOI: 10.1007/s40265-022-01826-9
Immune Mechanisms in Epileptogenesis: Update on Diagnosis and Treatment of Autoimmune Epilepsy Syndromes
Abstract
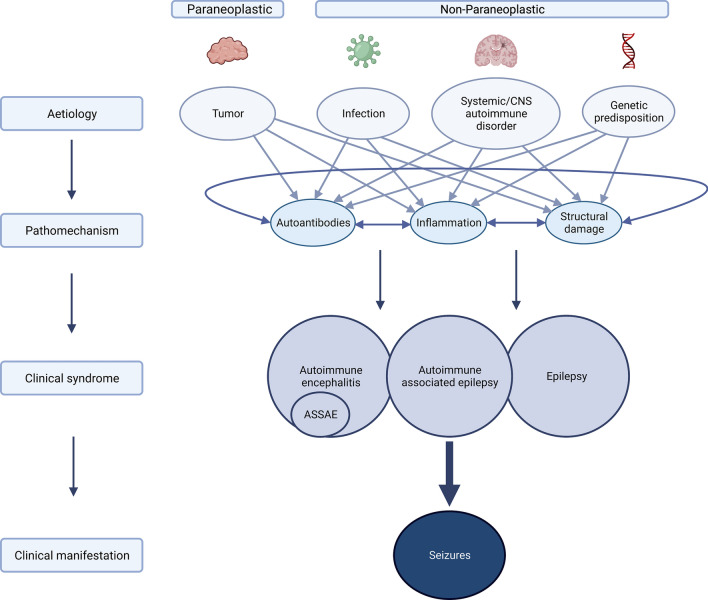
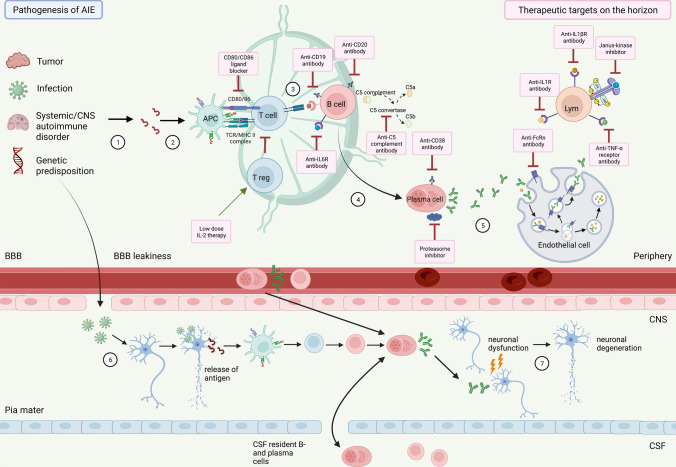
Seizures and epilepsy can result from various aetiologies, yet the underlying cause of several epileptic syndromes remains unclear. In that regard, autoimmune-mediated pathophysiological mechanisms have been gaining attention in the past years and were included as one of the six aetiologies of seizures in the most recent classification of the International League Against Epilepsy. The increasing number of anti-neuronal antibodies identified in patients with encephalitic disorders has contributed to the establishment of an immune-mediated pathophysiology in many cases of unclear aetiology of epileptic syndromes. Yet only a small number of patients with autoimmune encephalitis develop epilepsy in the proper sense where the brain transforms into a state where it will acquire the enduring propensity to produce seizures if it is not hindered by interventions. Hence, the term autoimmune epilepsy is often wrongfully used in the context of autoimmune encephalitis since most of the seizures are acute encephalitis-associated and will abate as soon as the encephalitis is in remission. Given the overlapping clinical presentation of immune-mediated seizures originating from different aetiologies, a clear distinction among the aetiological entities is crucial when it comes to discussing pathophysiological mechanisms, therapeutic options, and long-term prognosis of patients. Moreover, a rapid and accurate identification of patients with immune-mediated epilepsy syndromes is required to ensure an early targeted treatment and, thereby, improve clinical outcome. In this article, we review our current understanding of pathogenesis and critically discuss current and potential novel treatment options for seizures and epilepsy syndromes of underlying or suspected immune-mediated origin. We further outline the challenges in proper terminology.
© 2023. The Author(s).
Conflict of interest statement
A-K.P. has received speaker honoraria, research support or research/travel support from Roche and Biogen all used for research and without influence on the manuscript. S.R. has received funding from the Swiss National Science Foundation (grant number 320030_169379/1 and co-applicant for grant numbers 33CM30_125115/1 and 33CM30_140338/1, and from UCB-pharma. He has received honoraria from serving on the scientific advisory boards of Arvelle/Angelini, Bial, Eisai, GW, and UCB-pharma, and from serving as a consultant for Arvelle/Angelini, Eisai, Jazz Pharmaceuticals, Pfizer, Novartis, Sandoz, and UCB-pharma. He has received speaker’s honoraria from Eisai and Novartis. He does not hold any stocks of any pharmaceutical industries or manufacturers of medical devices. He disclosed that he is the past-president of the Swiss League against Epilepsy (no payments), Editor-in-chief of Zeitschrift für Epileptologie/ Clinical Epileptology (from 2023) (no payments). J.F., T.N. declare that they have no conflict of interest.
Figures
Similar articles
-
Acute symptomatic seizures secondary to autoimmune encephalitis and autoimmune-associated epilepsy: Conceptual definitions.Epilepsia. 2020 Jul;61(7):1341-1351. doi: 10.1111/epi.16571. Epub 2020 Jun 16. Epilepsia. 2020. PMID: 32544279 Review.
-
Autoimmune epilepsy in children: case series and proposed guidelines for identification.Epilepsia. 2013 Jun;54(6):1036-45. doi: 10.1111/epi.12142. Epub 2013 Mar 28. Epilepsia. 2013. PMID: 23551014
-
What is autoimmune encephalitis-associated epilepsy? Proposal of a practical definition.Epilepsia. 2023 Sep;64(9):2249-2255. doi: 10.1111/epi.17699. Epub 2023 Jul 25. Epilepsia. 2023. PMID: 37353891
-
Autoimmune and paraneoplastic seizures.Handb Clin Neurol. 2024;200:151-172. doi: 10.1016/B978-0-12-823912-4.00009-8. Handb Clin Neurol. 2024. PMID: 38494275 Review.
-
Autoimmune-associated epilepsy - a challenging concept.Seizure. 2025 May;128:20-23. doi: 10.1016/j.seizure.2024.05.017. Epub 2024 May 27. Seizure. 2025. PMID: 38852019 Review.
Cited by
-
The Role of Neuroinflammation and Network Anomalies in Drug-Resistant Epilepsy.Neurosci Bull. 2025 May;41(5):881-905. doi: 10.1007/s12264-025-01348-w. Epub 2025 Feb 24. Neurosci Bull. 2025. PMID: 39992353 Free PMC article. Review.
-
Cenobamate and Clobazam Combination as Personalized Medicine in Autoimmune-Associated Epilepsy With Anti-Gad65 Antibodies.Neurol Neuroimmunol Neuroinflamm. 2023 Aug 22;10(6):e200151. doi: 10.1212/NXI.0000000000200151. Print 2023 Nov. Neurol Neuroimmunol Neuroinflamm. 2023. PMID: 37607753 Free PMC article.
-
Wireless EEG Recording of Audiogenic Seizure Activity in Freely Moving Krushinsky-Molodkina Rats.Biomedicines. 2024 Apr 24;12(5):946. doi: 10.3390/biomedicines12050946. Biomedicines. 2024. PMID: 38790907 Free PMC article.
-
The causal relationship between immune cell traits and schizophrenia: a Mendelian randomization analysis.Front Immunol. 2024 Sep 27;15:1452214. doi: 10.3389/fimmu.2024.1452214. eCollection 2024. Front Immunol. 2024. PMID: 39399496 Free PMC article.
-
Genetic causal role of body mass index in multiple neurological diseases.Sci Rep. 2024 Mar 27;14(1):7256. doi: 10.1038/s41598-024-57260-2. Sci Rep. 2024. PMID: 38538647 Free PMC article.
References
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
