

Economic costs and cost-effectiveness of conditional cash transfers for the uptake of services for the prevention of vertical HIV transmissions in a resource-limited setting
- PMID: 36696797
- PMCID: PMC9975037
- DOI: 10.1016/j.socscimed.2023.115684
Economic costs and cost-effectiveness of conditional cash transfers for the uptake of services for the prevention of vertical HIV transmissions in a resource-limited setting
Abstract
Background: Prevention of mother-to-child transmission (PMTCT) is critical for halting the HIV epidemic. However, innovative approaches to improve PMTCT uptake may be resource-intensive. We examined the economic costs and cost-effectiveness of conditional cash transfers (CCTs) for the uptake of PMTCT services in the Democratic Republic of Congo.
Methods: We leveraged data from a randomized controlled trial of CCTs (n = 216) versus standard PMTCT care alone (standard of care (SOC), n = 217). Economic cost data came from multiple sources, with costs analyzed from the societal perspective and reported in 2016 international dollars (I$). Effectiveness outcomes included PMTCT uptake (i.e., accepting all PMTCT visits and services) and retention (i.e., in HIV care at six weeks post-partum). Generalized estimating equations estimated effectiveness (relative risk) and incremental costs, with incremental effectiveness reported as the number of women needing CCTs for an additional PMTCT uptake or retention. We evaluated the cost-effectiveness of the CCTs at various levels of willingness-to-pay and assessed uncertainty using deterministic sensitivity analysis and cost-effectiveness acceptability curves.
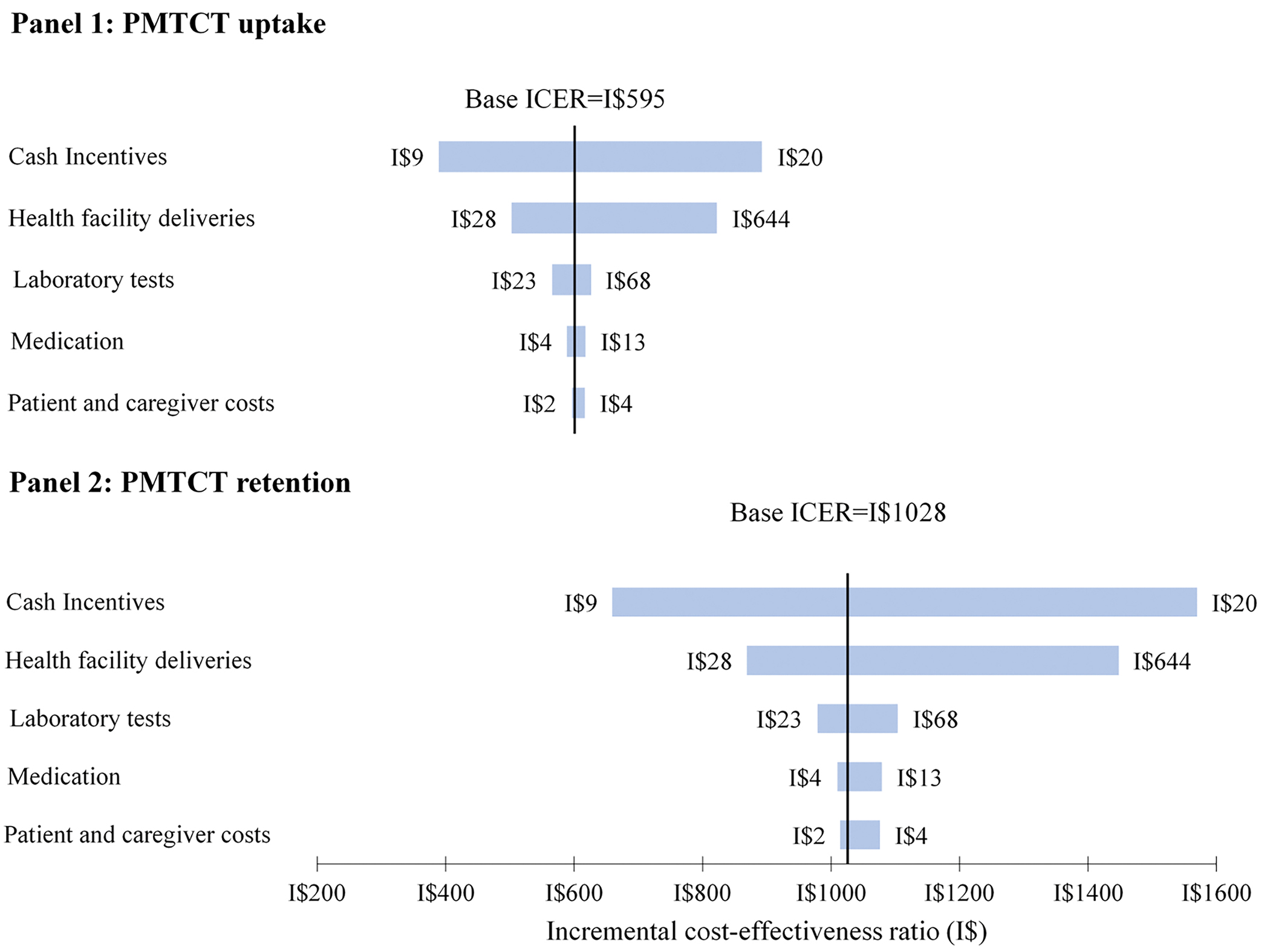
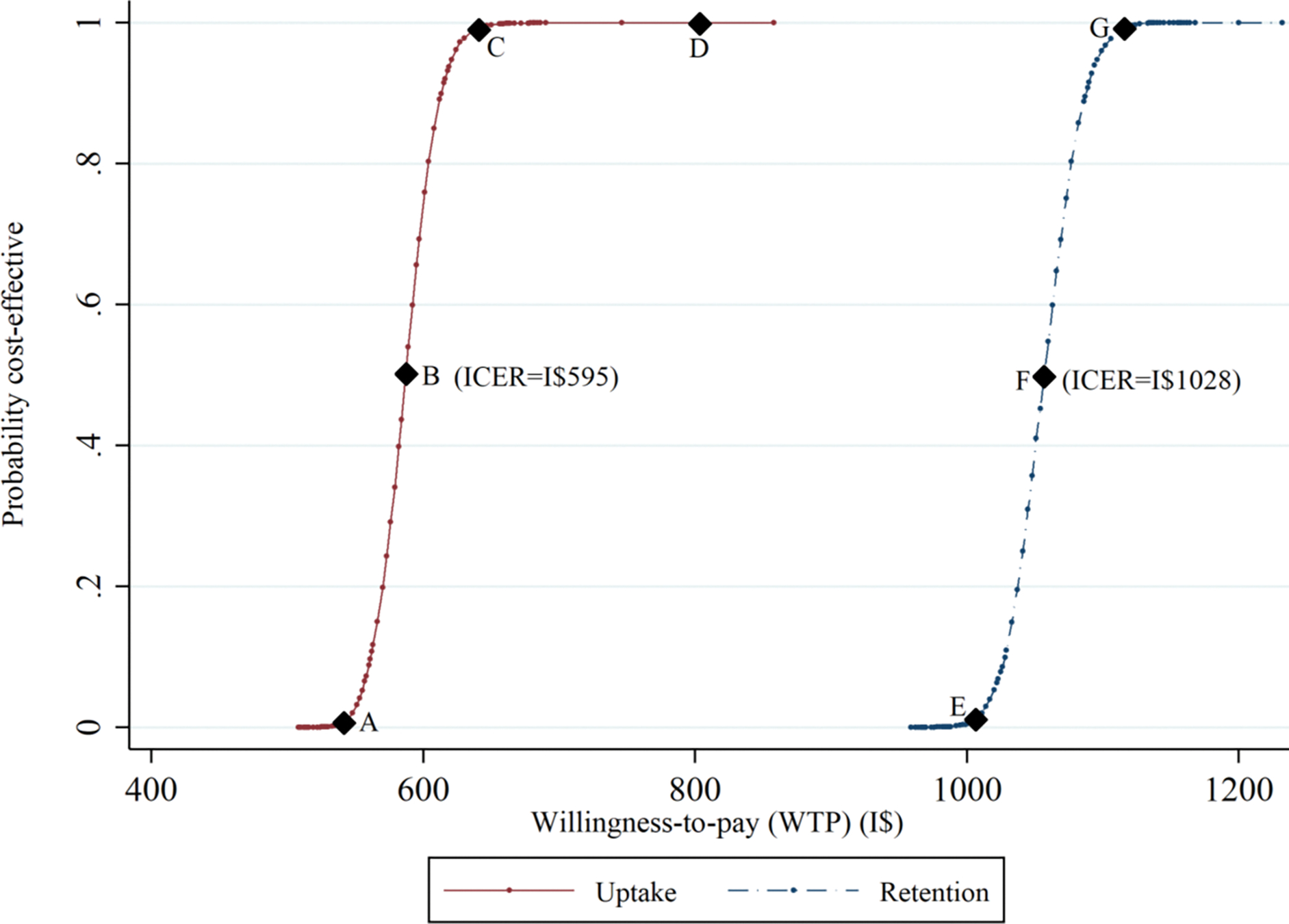
Results: Mean costs per participant were I$516 (CCTs) and I$431 (SOC), representing an incremental cost of I$85 (95% CI: 59, 111). PMTCT uptake was more likely for CCTs vs SOC (68% vs 53%, p < 0.05), with seven women needing CCTs for each additional PMTCT service uptake; twelve women needed CCTs for an additional PMTCT retention. The incremental cost-effectiveness of CCTs vs SOC was I$595 (95% CI: I$550, I$638) for PMTCT uptake and I$1028 (95% CI: I$931, I$1125) for PMTCT retention. CCTs would be an efficient use of resources if society's willingness-to-pay for an additional woman who takes up PMTCT services is at least I$640. In the worst-case scenario, the findings remained relatively robust.
Conclusions: Given the relatively low cost of the CCTs, policies supporting CCTs may decrease onward HIV transmission and expedite progress toward ending the epidemic.
Keywords: Conditional cash transfers; Cost-effectiveness; Economic costs; HIV; PMTCT; Retention; The Democratic Republic of the Congo; Uptake.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Conditional cash transfers and uptake of and retention in prevention of mother-to-child HIV transmission care: a randomised controlled trial.Lancet HIV. 2016 Feb;3(2):e85-93. doi: 10.1016/S2352-3018(15)00247-7. Lancet HIV. 2016. PMID: 26847230 Free PMC article. Clinical Trial.
-
The economic costs and cost-effectiveness of HIV self-testing among truck drivers in Kenya.Health Policy Plan. 2024 Apr 10;39(4):355-362. doi: 10.1093/heapol/czae013. Health Policy Plan. 2024. PMID: 38441272 Free PMC article. Clinical Trial.
-
Conditional Cash Transfers to Increase Retention in PMTCT Care, Antiretroviral Adherence, and Postpartum Virological Suppression: A Randomized Controlled Trial.J Acquir Immune Defic Syndr. 2016 Aug 1;72 Suppl 2(Suppl 2):S124-9. doi: 10.1097/QAI.0000000000001062. J Acquir Immune Defic Syndr. 2016. PMID: 27355499 Free PMC article. Clinical Trial.
-
Socio-Structural Factors Influencing the Prevention of Mother-to-Child Transmission of HIV in the Democratic Republic of the Congo: A Systematic Review.Matern Child Health J. 2019 Jul;23(7):880-889. doi: 10.1007/s10995-018-2688-6. Matern Child Health J. 2019. PMID: 30600507
-
Option B+ for the prevention of mother-to-child transmission of HIV infection in developing countries: a review of published cost-effectiveness analyses.Health Policy Plan. 2016 Oct;31(8):1133-41. doi: 10.1093/heapol/czw025. Epub 2016 Mar 26. Health Policy Plan. 2016. PMID: 27016949 Review.
Cited by
-
Understanding effective post-test linkage strategies for HIV prevention and care: a scoping review.J Int AIDS Soc. 2024 Apr;27(4):e26229. doi: 10.1002/jia2.26229. J Int AIDS Soc. 2024. PMID: 38604993 Free PMC article.
-
Cash transfer, maternal and child health outcomes: a scoping review in sub-Saharan Africa.Glob Health Action. 2024 Dec 31;17(1):2309726. doi: 10.1080/16549716.2024.2309726. Epub 2024 Feb 9. Glob Health Action. 2024. PMID: 38333923 Free PMC article.
-
Cost-Effectiveness of Using Conditional Economic Incentives to Improve Pre-exposure Prophylaxis Adherence Among Male Sex Workers.Pharmacoecon Open. 2025 Jul;9(4):649-659. doi: 10.1007/s41669-025-00569-z. Epub 2025 Apr 9. Pharmacoecon Open. 2025. PMID: 40205318 Free PMC article.
References
-
- UNAIDS . Start Free Stay Free AIDS Free — 2017 progress report 2018. [Available from: http://www.unaids.org/en/resources/documents/2018/start-free-stay-free-a...]. Accessed 14 April 2018.
-
- UNAIDS. How AIDS changed everything 2015. [updated 2015. Available from: http://www.unaids.org/sites/default/files/media_asset/MDG6Report_en.pdf]. Accessed.
-
- UNAIDS. Country factsheets: Democratic Republic of the Congo, 2021 2021. [cited 2022 17 November]. Available from: https://aidsinfo.unaids.org/]. Accessed 15 November 2022.
-
- World Health Organization. Treat all people living with HIV, offer antiretrovirals as additional prevention choice for people at “substantial” risk 2015. [Available from: https://www.who.int/mediacentre/news/releases/2015/hiv-treat-all-recomme...]. Accessed 18 March 2017.
-
- Maartens G, Celum C, Lewin SR. HIV infection: epidemiology, pathogenesis, treatment, and prevention. Lancet (London, England). 2014;384(9939):258–71. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
