

Using body cameras to quantify the duration of a Code Stroke and identify workflow issues: a continuous observation workflow time study
- PMID: 36697041
- PMCID: PMC9884893
- DOI: 10.1136/bmjopen-2022-067816
Using body cameras to quantify the duration of a Code Stroke and identify workflow issues: a continuous observation workflow time study
Abstract
Objective: 'Code Stroke' (Code) is used in health services to streamline hyperacute assessment and treatment delivery for patients with ischaemic stroke. However, there are few studies that detail the time spent on individual components performed during a Code. We sought to quantify the time taken for each process during a Code and investigate associations with modifiable and non-modifiable factors.
Design: Continuous observation workflow time study.
Setting and participants: Recordings of 100 Codes were performed at a high-volume primary stroke centre in Melbourne, Australia, between January and June 2020 using a body camera worn by a member of the stroke team.
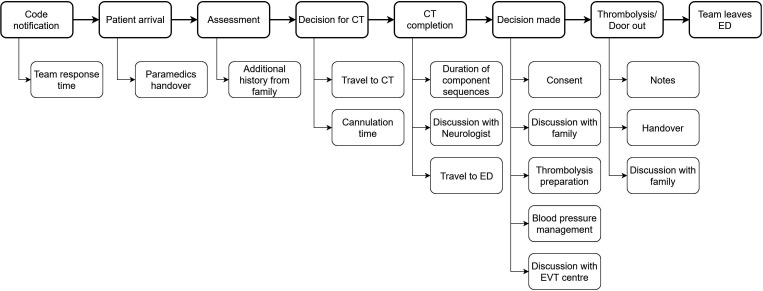
Main outcome measures: The main measures included the overall duration of Codes and the individual processes within the Code workflow. Associations between variables of interest and process times were explored using linear regression models.
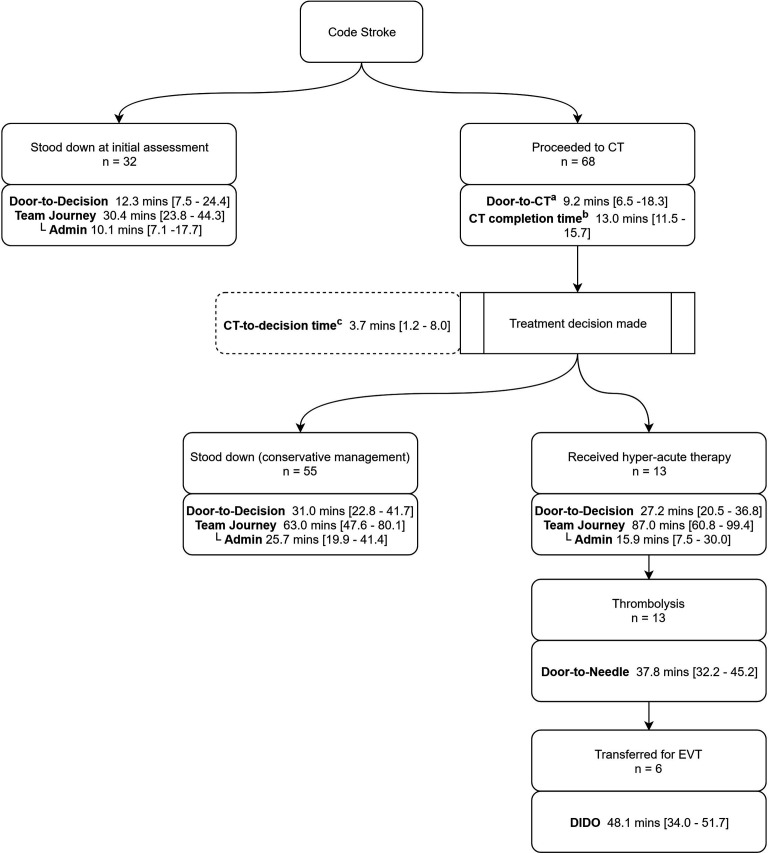
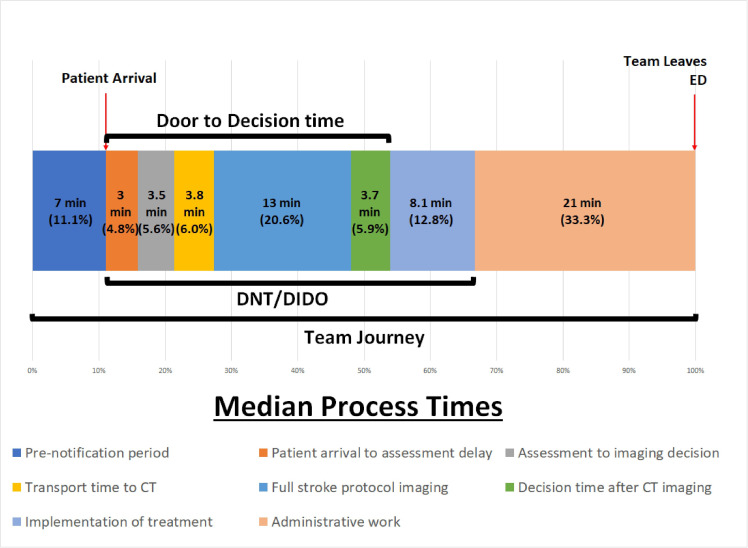
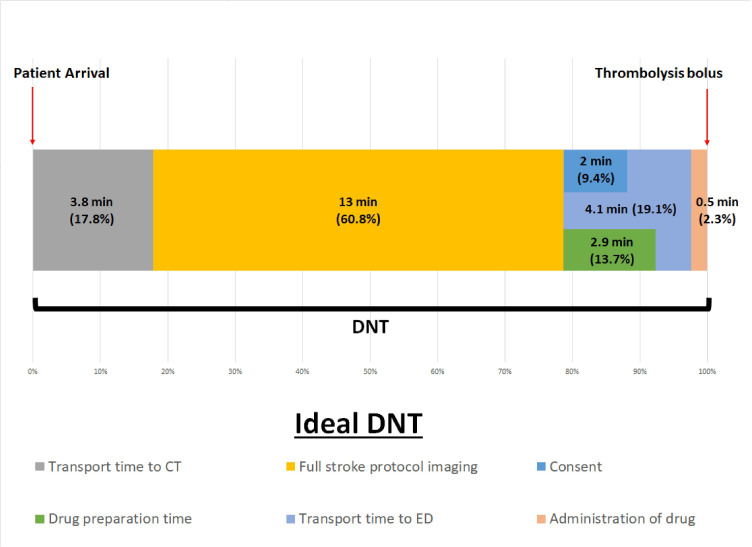
Results: 100 Codes were captured, representing 19.2% of all Codes over the 6 months. The median duration of a complete Code was 54.2 min (IQR 39.1-74.7). Administrative work performed after treatment is completed (median 21.0 min (IQR 9.8-31.4)); multimodal CT imaging (median 13.0 min (IQR 11.5-15.7)), and time between decision and thrombolysis administration (median 8.1 min (IQR 6.1-10.8)) were the longest components of a Code. Tenecteplase was able to be prepared faster than alteplase (median 1.8 vs 4.9 min, p=0.02). The presence of a second junior doctor was associated with shorter administrative work time (median 10.3 vs 25.1 min, p<0.01). No specific modifiable factors were found to be associated with shorter overall Code duration.
Conclusions: Codes are time intensive. Time spent on decision-making was a relatively small component of the overall Code duration. Data from body cameras can provide granular data on all aspects of Code workflow to inform potential areas for improvement at individual centres.
Keywords: Clinical audit; STROKE MEDICINE; Stroke.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
The quest to reduce stroke treatment delays at a Melbourne metropolitan primary stroke centre over the past two decades.Intern Med J. 2022 Nov;52(11):1978-1985. doi: 10.1111/imj.15429. Epub 2022 Jun 13. Intern Med J. 2022. PMID: 34142750
-
Comparison of tenecteplase with alteplase for the early treatment of ischaemic stroke in the Melbourne Mobile Stroke Unit (TASTE-A): a phase 2, randomised, open-label trial.Lancet Neurol. 2022 Jun;21(6):520-527. doi: 10.1016/S1474-4422(22)00171-5. Epub 2022 May 4. Lancet Neurol. 2022. PMID: 35525251 Clinical Trial.
-
Hyperacute stroke thrombolysis via telemedicine: a multicentre study of performance, safety and clinical efficacy.BMJ Open. 2022 Jan 17;12(1):e057372. doi: 10.1136/bmjopen-2021-057372. BMJ Open. 2022. PMID: 35039306 Free PMC article.
-
Extending thrombolysis to 4·5-9 h and wake-up stroke using perfusion imaging: a systematic review and meta-analysis of individual patient data.Lancet. 2019 Jul 13;394(10193):139-147. doi: 10.1016/S0140-6736(19)31053-0. Epub 2019 May 22. Lancet. 2019. PMID: 31128925
-
Acute Treatment of Ischemic Stroke.Neurol Clin. 2022 Feb;40(1):17-32. doi: 10.1016/j.ncl.2021.08.002. Neurol Clin. 2022. PMID: 34798968 Review.
Cited by
-
Streamlining Acute Stroke Processes and Data Collection: A Narrative Review.Healthcare (Basel). 2024 Sep 25;12(19):1920. doi: 10.3390/healthcare12191920. Healthcare (Basel). 2024. PMID: 39408100 Free PMC article. Review.
References
-
- Emberson J, Lees KR, Lyden P, et al. . Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet 2014;384:1929–35. 10.1016/S0140-6736(14)60584-5 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical