

Fixed dose combination drugs for cardiovascular disease in a prolonged humanitarian crisis in Lebanon: an implementation study
- PMID: 36697043
- PMCID: PMC9884866
- DOI: 10.1136/bmjopen-2022-063668
Fixed dose combination drugs for cardiovascular disease in a prolonged humanitarian crisis in Lebanon: an implementation study
Abstract
Objectives: This pre-post implementation study evaluated the introduction of fixed dose combination (FDC) medications for atherosclerotic cardiovascular disease (ASCVD) secondary prevention into routine care in a humanitarian setting.
Setting: Two Médecins sans Frontières (MSF) primary care clinics serving Syrian refugee and host populations in north Lebanon.
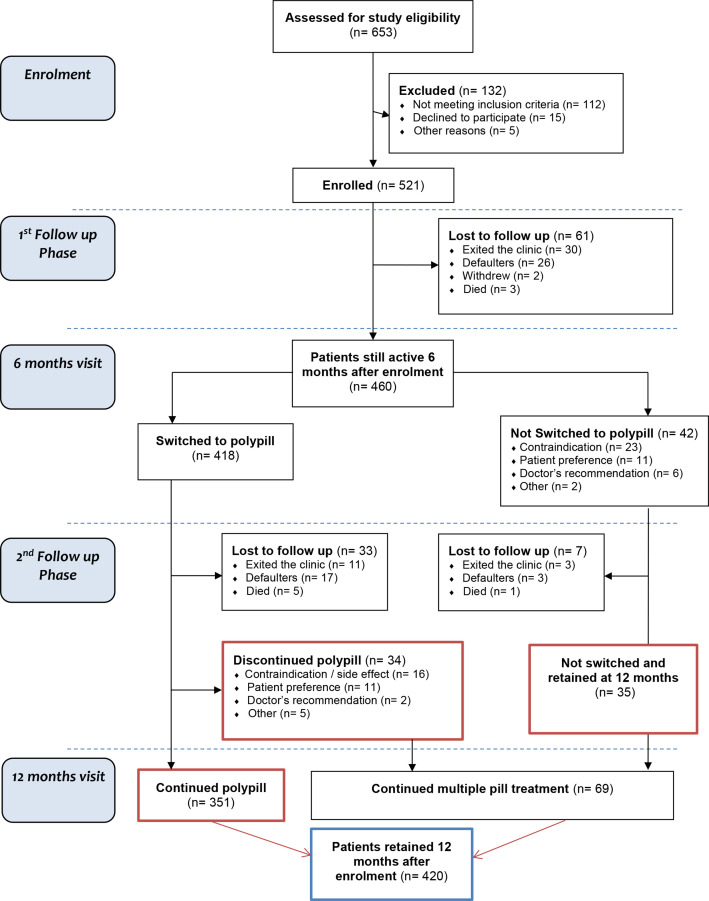
Participants: Consenting patients ≥18 years with existing ASCVD requiring secondary prevention medication were eligible for study enrolment. Those with FDC contraindication(s) or planning to move were excluded. Of 521 enrolled patients, 460 (88.3%) were retained at 6 months, and 418 (80.2%) switched to FDC. Of these, 84% remained on FDC (n=351), 8.1% (n=34) discontinued and 7.9% (n=33) were lost to follow-up by month 12.
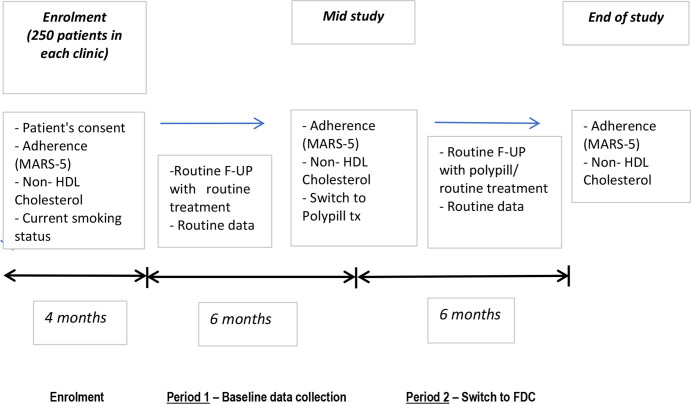
Interventions: Eligible patients, enrolled February-May 2019, were switched to Trinomia FDC (atorvastatin 20 mg, aspirin 100 mg, ramipril 2.5/5/10 mg) after 6 months' usual care. During the study, the COVID-19 pandemic, an economic crisis and clinic closures occurred.
Outcome measures: Descriptive and regression analyses compared key outcomes at 6 and 12 months: medication adherence, non-high density lipoprotein cholesterol (non-HDL-C) and systolic blood pressure (SBP) control. We performed per-protocol, intention-to-treat and secondary analyses of non-switchers.
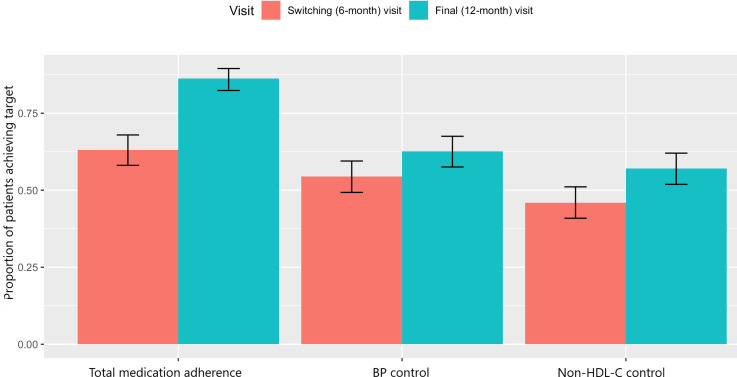
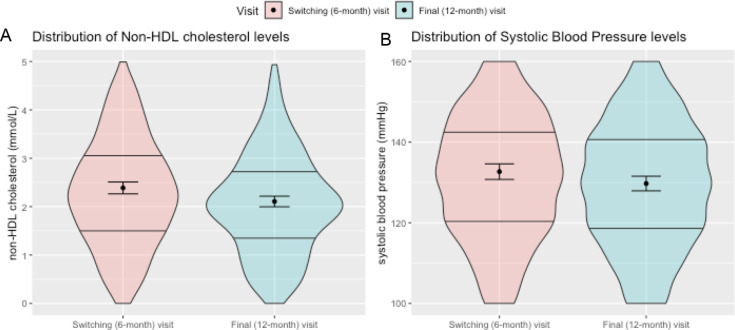
Results: Among 385 switchers remaining at 12 months, total adherence improved 23%, from 63% (95% CI 58 to 68) at month 6, to 86% (95% CI 82 to 90) at month 12; mean non-HDL-C levels dropped 0.28 mmol/L (95% CI -0.38 to -0.18; p<0.0001), from 2.39 (95% CI 2.26 to 2.51) to 2.11 mmol/L (95% CI 2.00 to 2.22); mean SBP dropped 2.89 mm Hg (95% CI -4.49 to -1.28; p=0.0005) from 132.7 (95% CI 130.8 to 134.6) to 129.7 mm Hg (95% CI 127.9 to 131.5). Non-switchers had smaller improvements in adherence and clinical outcomes.
Conclusion: Implementing an ASCVD secondary prevention FDC improved adherence and CVD risk factors in MSF clinics in Lebanon, with potential for wider implementation by humanitarian actors and host health systems.
Keywords: Ischaemic heart disease; PREVENTIVE MEDICINE; PRIMARY CARE; PUBLIC HEALTH; THERAPEUTICS.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Implementation of fixed-dose combination therapy for secondary prevention of atherosclerotic cardiovascular disease among Syrian refugees in Lebanon: a qualitative evaluation.BMC Health Serv Res. 2022 Jun 4;22(1):744. doi: 10.1186/s12913-022-08040-z. BMC Health Serv Res. 2022. PMID: 35659222 Free PMC article.
-
Cardiovascular Disease among Syrian refugees: a descriptive study of patients in two Médecins Sans Frontières clinics in northern Lebanon.Confl Health. 2019 Aug 9;13:37. doi: 10.1186/s13031-019-0217-x. eCollection 2019. Confl Health. 2019. PMID: 31413727 Free PMC article.
-
Effect of fixed dose combination treatment on adherence and risk factor control among patients at high risk of cardiovascular disease: randomised controlled trial in primary care.BMJ. 2014 May 27;348:g3318. doi: 10.1136/bmj.g3318. BMJ. 2014. PMID: 24868083 Clinical Trial.
-
Vegan dietary pattern for the primary and secondary prevention of cardiovascular diseases.Cochrane Database Syst Rev. 2021 Feb 25;2(2):CD013501. doi: 10.1002/14651858.CD013501.pub2. Cochrane Database Syst Rev. 2021. PMID: 33629376 Free PMC article.
-
Lowering Targeted Atherogenic Lipoprotein Cholesterol Goals for Patients at "Extreme" ASCVD Risk.Curr Diab Rep. 2019 Nov 21;19(12):146. doi: 10.1007/s11892-019-1246-y. Curr Diab Rep. 2019. PMID: 31754844 Review.
References
-
- WHO 2007, Prevention of Cardiovascular Disease . Guidelines for assessment and management of cardiovascular risk - Google Search [Internet]. Available: https://www.google.com/search?client=safari&rls=en&q=WHO+2007,+Preventio... [Accessed 09 Jan 2019].
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous