

Thromboprophylaxis in Patients With Fontan Circulation
- PMID: 36697138
- PMCID: PMC11040452
- DOI: 10.1016/j.jacc.2022.10.037
Thromboprophylaxis in Patients With Fontan Circulation
Abstract
Background: The optimal strategy for thromboprophylaxis in patients with a Fontan circulation is unknown.
Objectives: The aim of this study was to compare the efficacy and safety of aspirin, warfarin, and nonvitamin K oral anticoagulants (NOACs) in a network meta-analysis.
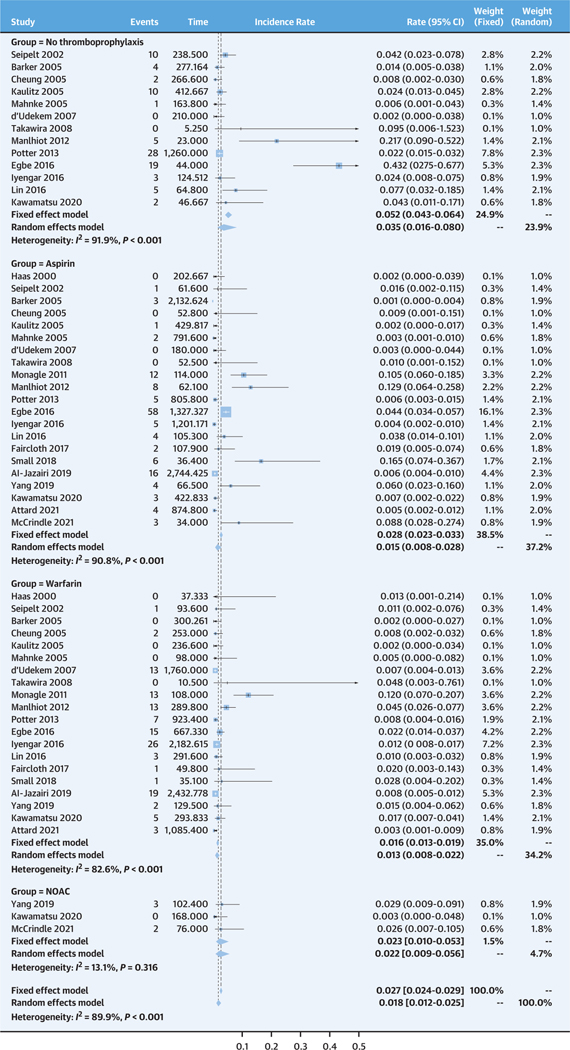
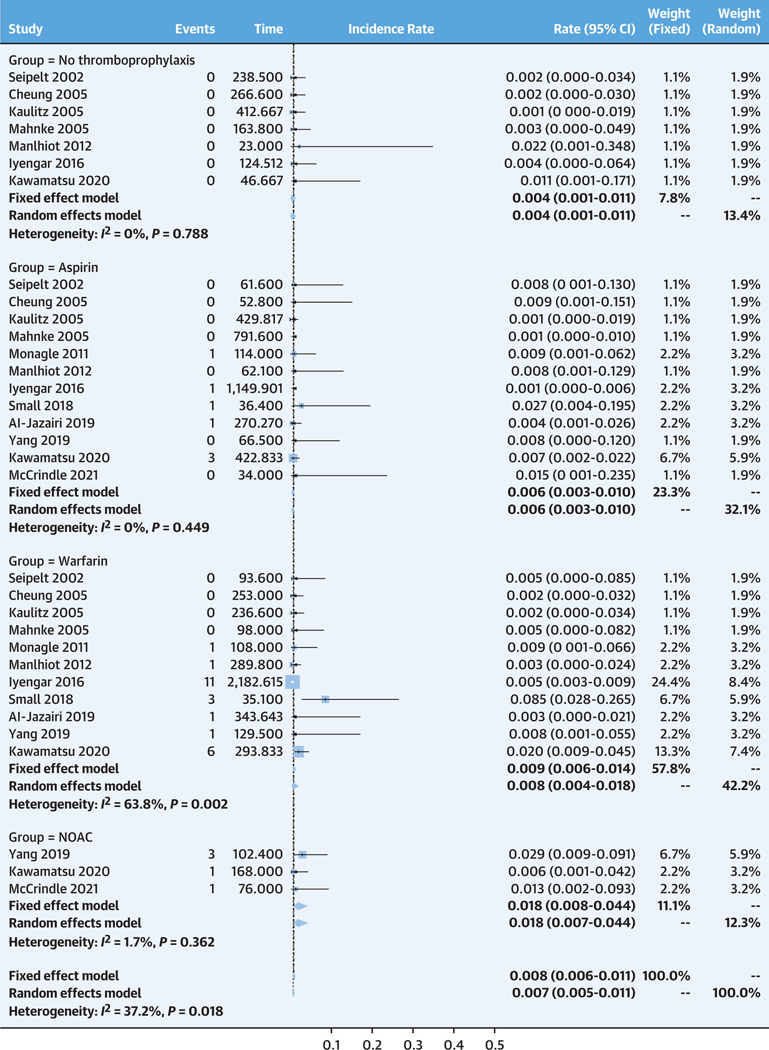
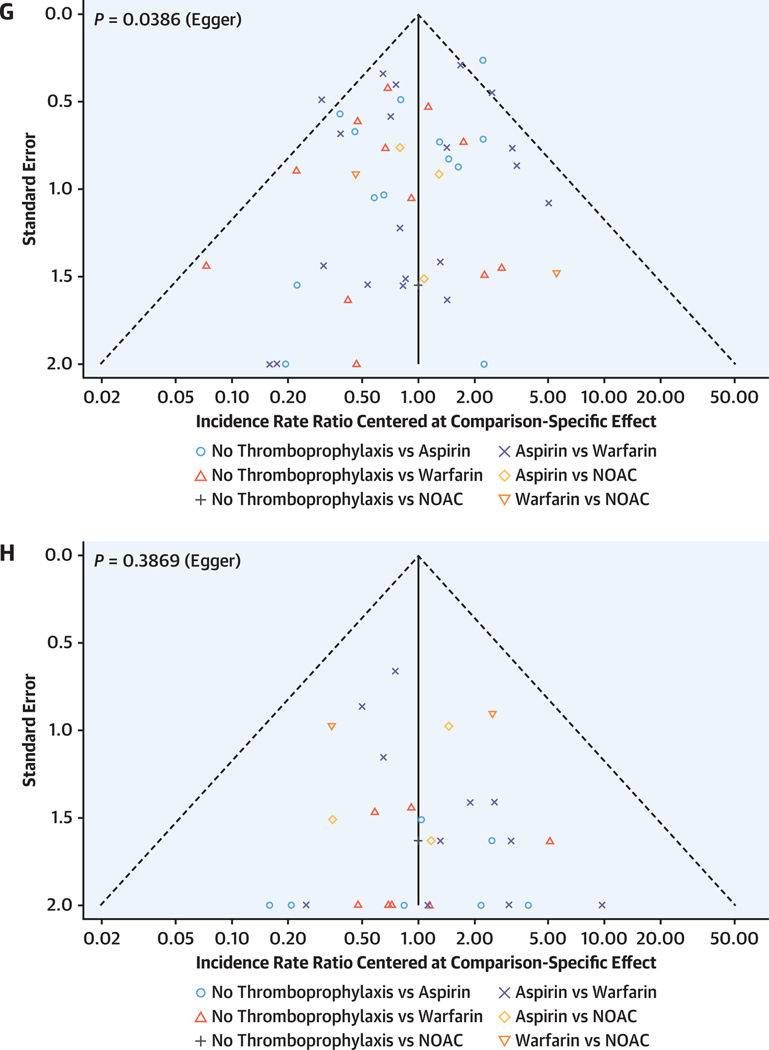
Methods: Relevant studies published by February 2022 were included. The primary efficacy outcome was thromboembolic events; major bleeding was a secondary safety outcome. Frequentist network meta-analyses were conducted to estimate the incidence rate ratios (IRRs) of both outcomes. Ranking of treatments was performed based on probability (P) score.
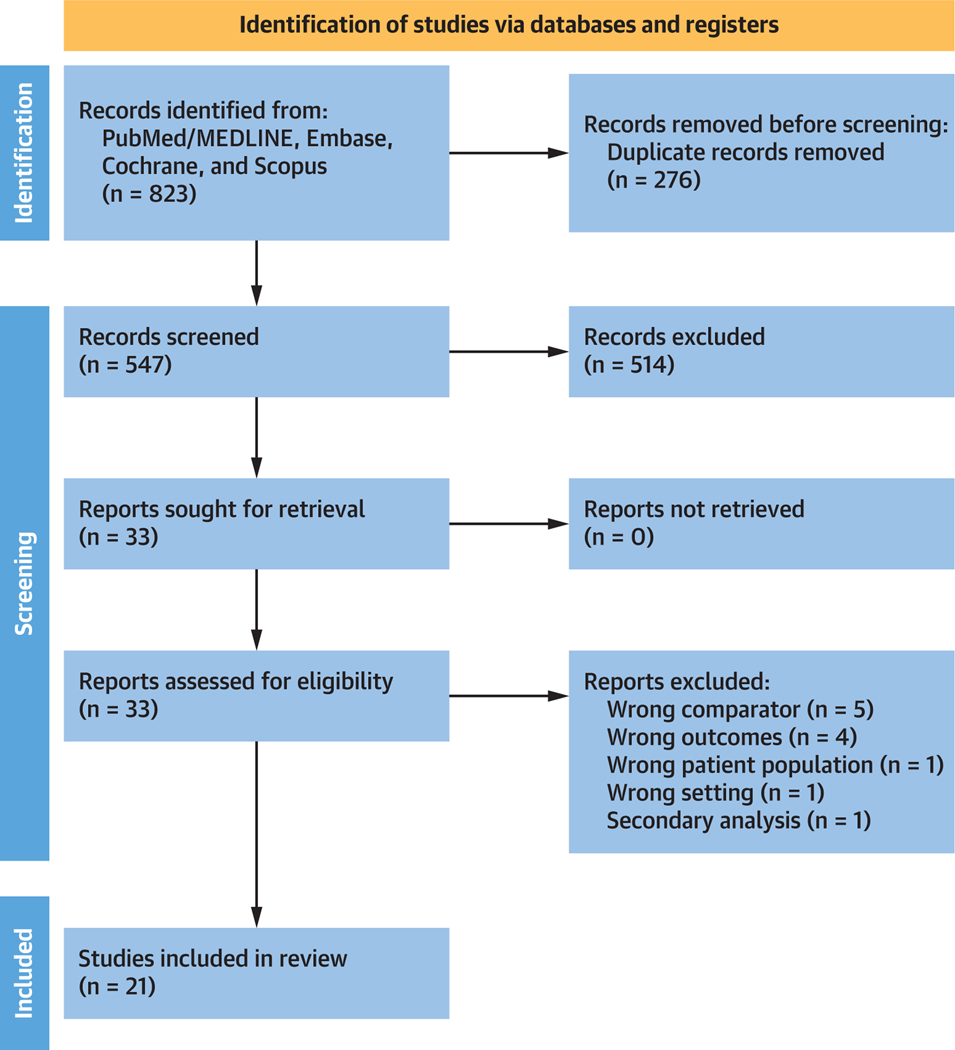
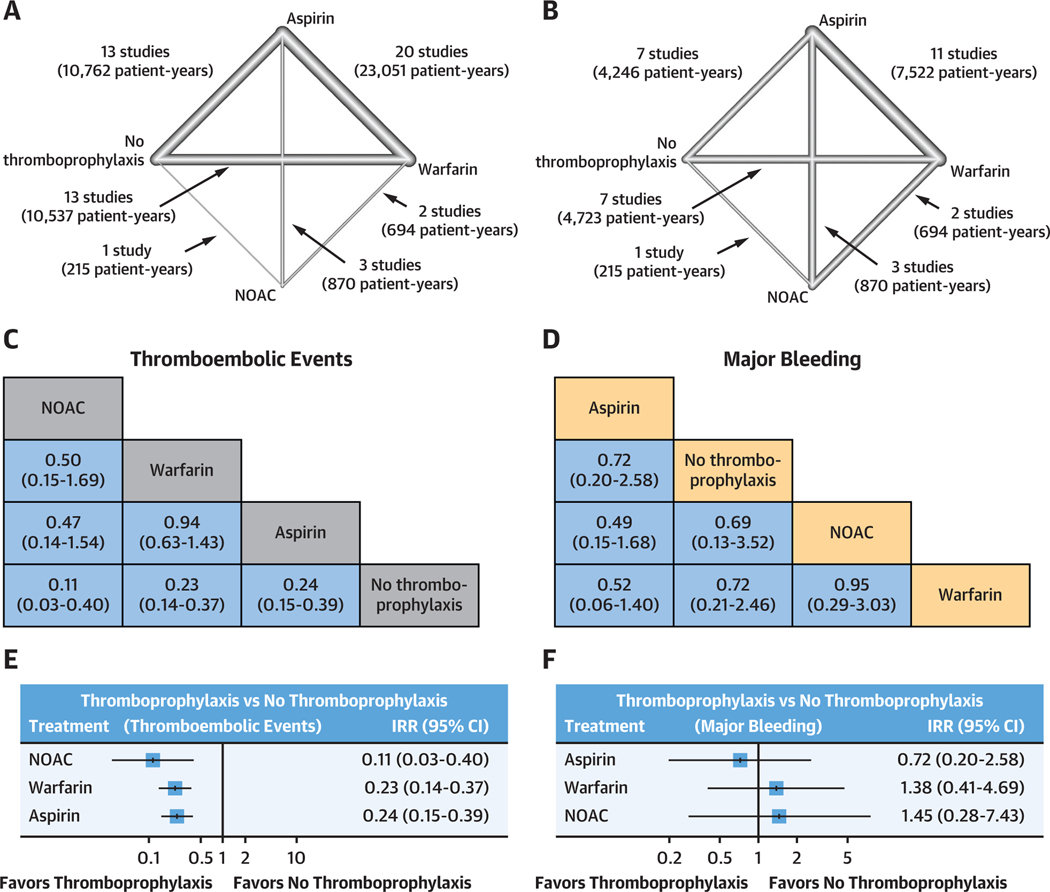
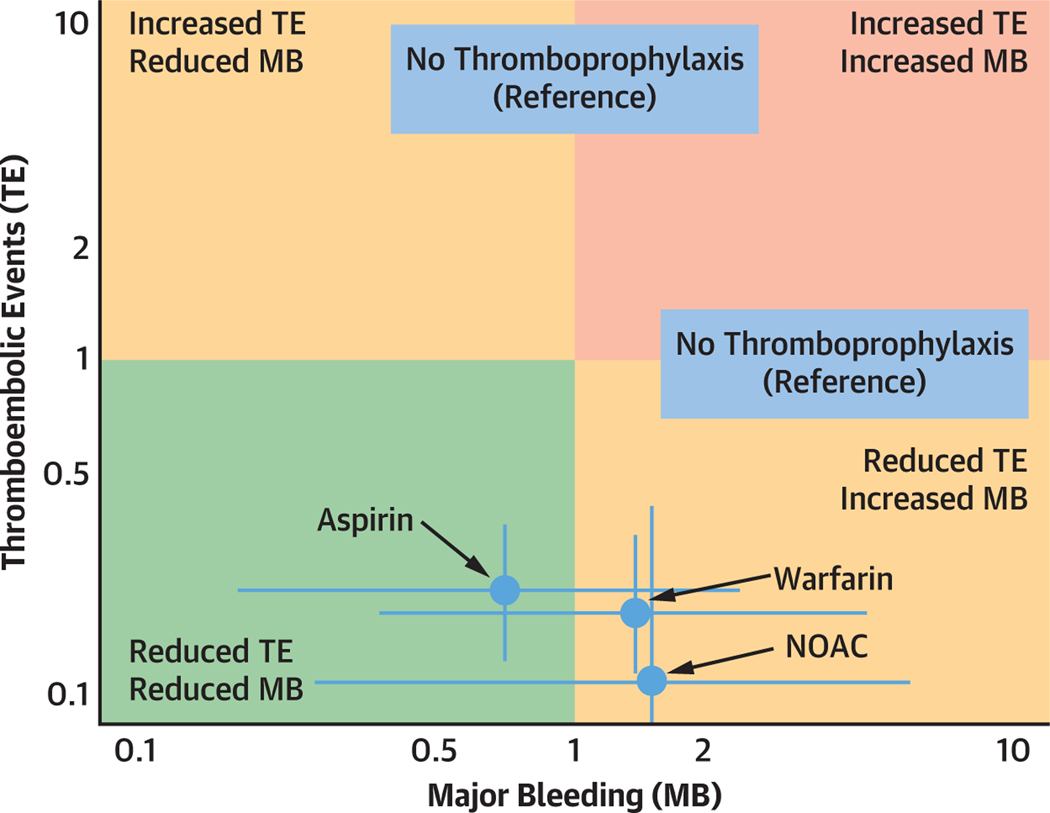
Results: A total of 21 studies were included (26,546 patient-years). When compared with no thromboprophylaxis, NOAC (IRR: 0.11; 95% CI: 0.03-0.40), warfarin (IRR: 0.23; 95% CI: 0.14-0.37), and aspirin (IRR: 0.24; 95% CI: 0.15-0.39) were all associated with significantly lower rates of thromboembolic events. However, the network meta-analysis revealed no significant differences in the rates of major bleeding (NOAC: IRR: 1.45 [95% CI: 0.28-7.43]; warfarin: IRR: 1.38 [95% CI: 0.41-4.69]; and aspirin: IRR: 0.72 [95% CI: 0.20-2.58]). Rankings, which simultaneously analyze competing interventions, suggested that NOACs have the highest P score to prevent thromboembolic events (P score 0.921), followed by warfarin (P score 0.582), aspirin (P score 0.498), and no thromboprophylaxis (P score 0.001). Aspirin tended to have the most favorable overall profile.
Conclusions: Aspirin, warfarin, and NOAC are associated with lower risk of thromboembolic events. Recognizing the limited number of patients and heterogeneity of studies using NOACs, the results support the safety and efficacy of NOACs in patients with a Fontan circulation.
Keywords: aspirin; nonvitamin K oral anticoagulants; single ventricle; warfarin.
Copyright © 2023 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Thromboprophylaxis in the Fontan Circulation: Long-Awaited Validation.J Am Coll Cardiol. 2023 Jan 31;81(4):390-393. doi: 10.1016/j.jacc.2022.11.029. J Am Coll Cardiol. 2023. PMID: 36697139 No abstract available.
References
-
- Pundi KN, Johnson JN, Dearani JA, et al. 40-year follow-up after the Fontan operation: long-term outcomes of 1,052 patients. J Am Coll Cardiol. 2015;66:1700–1710. - PubMed
-
- Dennis M, Zannino D, du Plessis K, et al. Clinical outcomes in adolescents and adults after the Fontan procedure. J Am Coll Cardiol. 2018;71: 1009–1017. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
