

Intracranial post-clipping residual or recurrent aneurysms: Current status and treatment options (Review)
- PMID: 36698683
- PMCID: PMC9855273
- DOI: 10.3892/mi.2021.1
Intracranial post-clipping residual or recurrent aneurysms: Current status and treatment options (Review)
Abstract
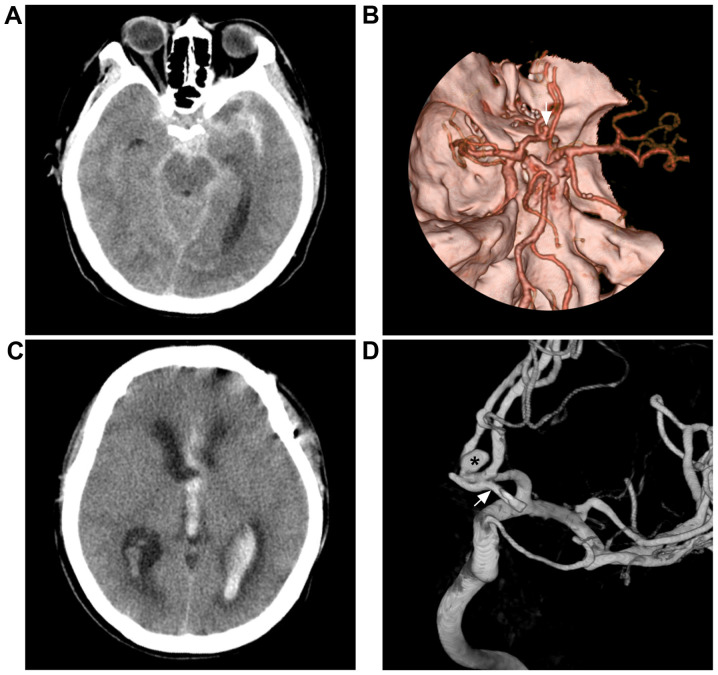
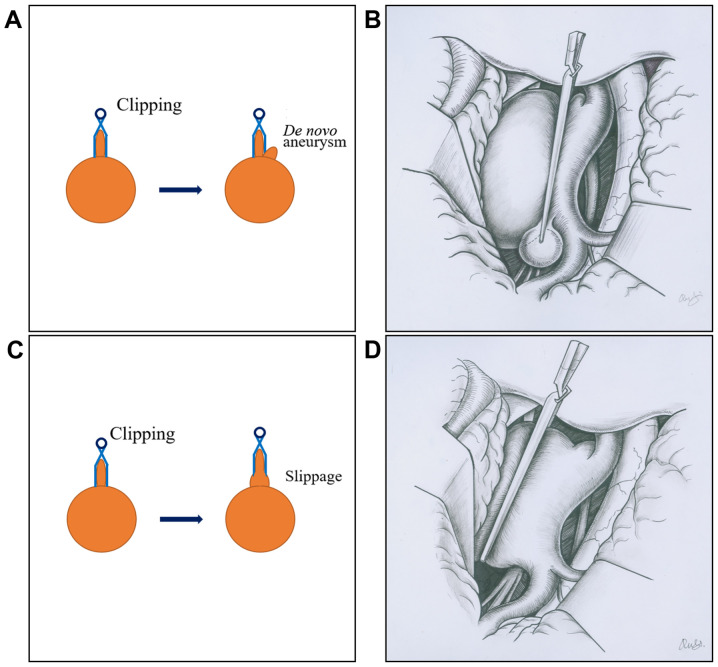
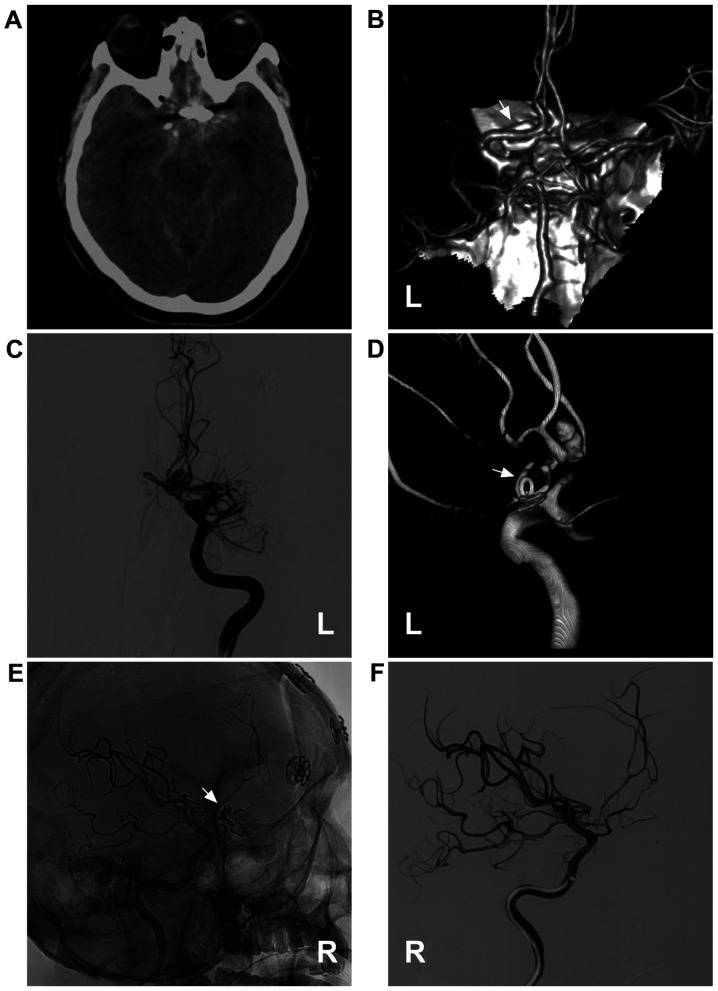
Following the clipping of intracranial aneurysms, post-clipping residual or recurrent aneurysms (PCRRAs) can occur. In recent years, the incidence of PCRRAs has increased due to a prolonged follow-up period and advanced imaging techniques. However, several aspects of intracranial PCRRAs remain unclear. Therefore, the present study performed an in-depth review of the literature on PCRRAs. Herein, a summary of PCRRAs that can be divided into the following two categories is presented: i) Those occurring after the incomplete clipping of an aneurysm, where the residual aneurysm regrows into a PCRRA; and ii) those occurring after the complete clipping of an aneurysm, in which a de novo aneurysm occurs at the original aneurysm site. Currently, digital subtracted angiography remains the gold standard for the imaging diagnosis of PCRRAs as it can eliminate metallic clip artifacts. Intracranial symptomatic PCRRAs should be actively treated, particularly those that have ruptured. A number of methods are currently available for the treatment of intracranial PCRRAs; these mainly include re-clipping, endovascular treatment (EVT) and bypass surgery. Currently, re-clipping remains the most effective method used to treat PCRRAs; however, it is a very difficult procedure to perform. EVT can also be used to treat intracranial PCRRAs. EVT methods include coiling (stent- or balloon-assisted) and flow-diverting stents (or coiling-assisted). Bypass surgery can be selected for difficult-to-treat, complex PCRRAs. On the whole, following appropriate treatment, the majority of intracranial PCRRAs achieve a high occlusion rate and a good prognosis.
Keywords: endovascular treatment; post-clipping residual or recurrent aneurysms; surgical treatment.
Copyright: © Piao et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Coil embolization for intracranial aneurysms: an evidence-based analysis.Ont Health Technol Assess Ser. 2006;6(1):1-114. Epub 2006 Jan 1. Ont Health Technol Assess Ser. 2006. PMID: 23074479 Free PMC article.
-
Important factors for a combined neurovascular team to consider in selecting a treatment modality for patients with previously clipped residual and recurrent intracranial aneurysms.Neurosurgery. 2003 Apr;52(4):732-8; discussion 738-9. doi: 10.1227/01.neu.0000053209.61909.f2. Neurosurgery. 2003. PMID: 12657168
-
Endovascular treatment of residual or recurrent intracranial aneurysms after surgical clipping.J Cerebrovasc Endovasc Neurosurg. 2021 Sep;23(3):221-232. doi: 10.7461/jcen.2021.E2021.03.001. Epub 2021 Sep 2. J Cerebrovasc Endovasc Neurosurg. 2021. PMID: 34470100 Free PMC article.
-
Secondary coiling after incomplete surgical clipping of cerebral aneurysms: a rescue strategy or a treatment option for complex cases? Institutional series and systematic review.Neurosurg Rev. 2019 Jun;42(2):337-350. doi: 10.1007/s10143-018-0950-4. Epub 2018 Feb 7. Neurosurg Rev. 2019. PMID: 29417290
-
Endovascular therapeutic strategies in ruptured intracranial aneurysms.Eur J Radiol. 2013 Oct;82(10):1646-52. doi: 10.1016/j.ejrad.2013.01.034. Epub 2013 Mar 21. Eur J Radiol. 2013. PMID: 23523515 Review.
Cited by
-
Intra-aneurysmal contrast agent stasis during intraoperative digital subtraction angiography may predict long-term occlusion after clipping.Acta Neurochir (Wien). 2024 Jul 30;166(1):309. doi: 10.1007/s00701-024-06162-3. Acta Neurochir (Wien). 2024. PMID: 39078422
-
Aggressive Behavior of Recurrent Middle Cerebral Artery Aneurysms: A Case Series.Cureus. 2024 Dec 26;16(12):e76435. doi: 10.7759/cureus.76435. eCollection 2024 Dec. Cureus. 2024. PMID: 39867010 Free PMC article.
-
The value of dual-energy computed tomography angiography-based virtual monoenergetic imaging for evaluations after cerebral aneurysm clipping.Diagn Interv Radiol. 2025 Apr 28;31(3):264-273. doi: 10.4274/dir.2024.242975. Epub 2024 Dec 16. Diagn Interv Radiol. 2025. PMID: 39676443 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources