

Isolated Adductor Magnus Injuries in Athletes: A Case Series
- PMID: 36698789
- PMCID: PMC9869219
- DOI: 10.1177/23259671221138806
Isolated Adductor Magnus Injuries in Athletes: A Case Series
Abstract
Background: Little is known about injuries to the adductor magnus (AM) muscle and how to manage them.
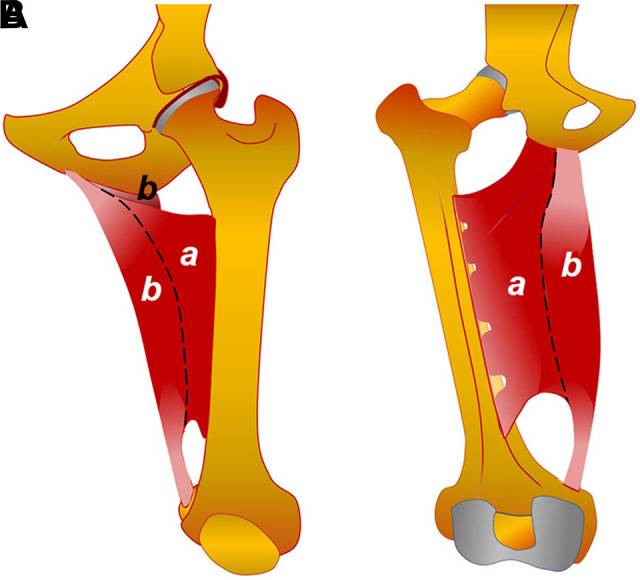
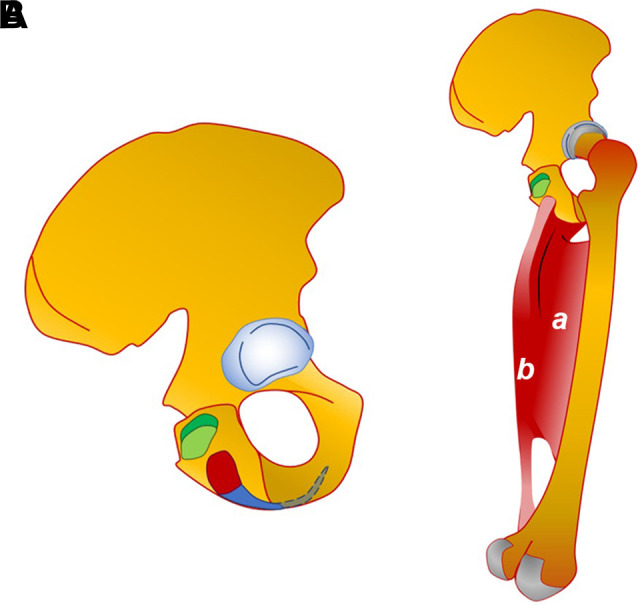
Purpose: To describe the injury mechanisms of the AM and its histoarchitecture, clinical characteristics, and imaging features in elite athletes.
Study design: Case series; Level of evidence, 4.
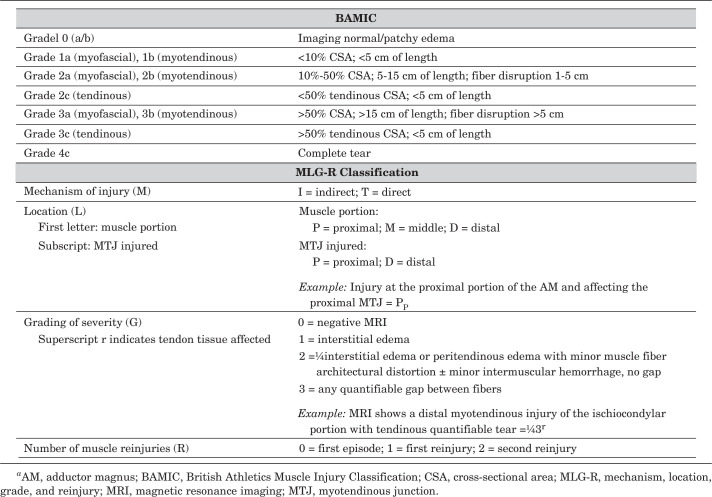
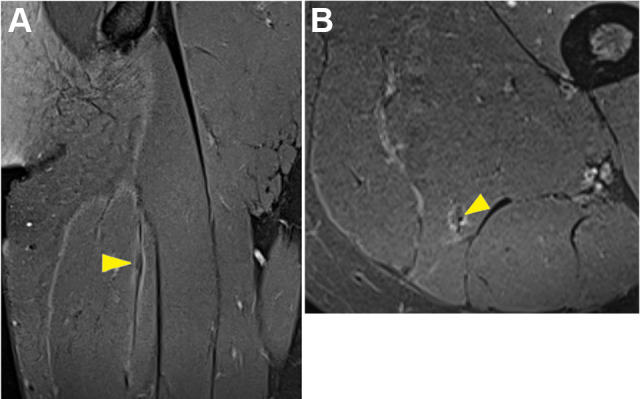
Methods: A total of 11 competitive athletes with an AM injury were included in the study. Each case was clinically assessed, and the diagnosis and classification were made by magnetic resonance imaging (MRI) according to the British Athletics Muscle Injury Classification (BAMIC) and mechanism, location, grade, and reinjury (MLG-R) classification. A 1-year follow-up was performed, and return-to-play (RTP) time was recorded.
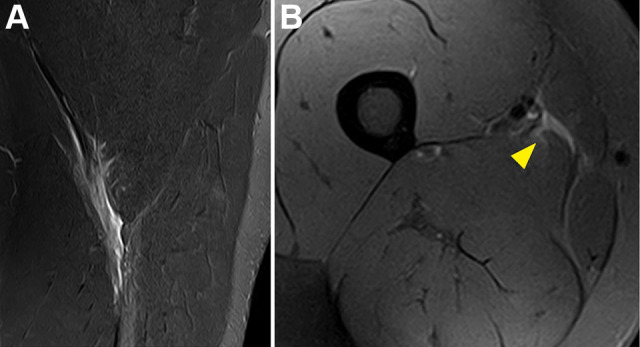
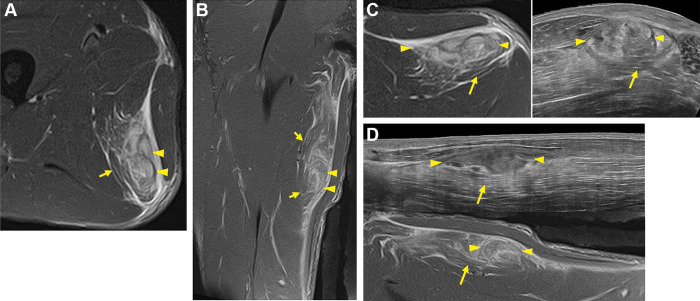
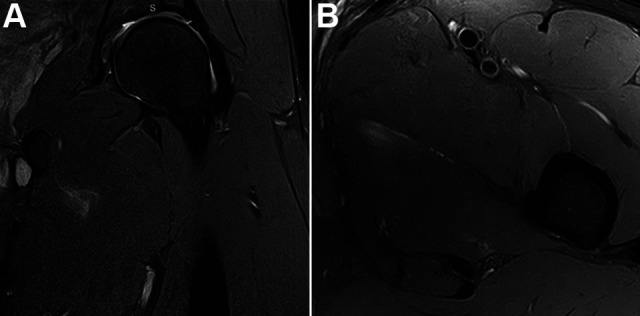
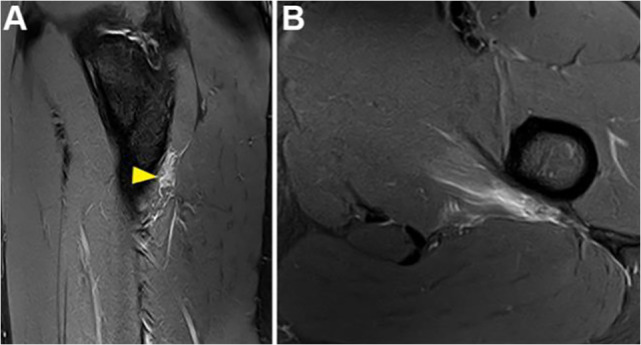
Results: Different mechanisms of injury were found; most of the athletes (10/11) had flexion and internal rotation of the hip with extension or slight flexion of the knee. Symptoms consisted of pain in the posteromedial (7/11) or medial (4/11) thigh during adduction and flexion of the knee. Clinically, there was a suspicion of an injury to the AM in only 3 athletes. According to MRI, 5 lesions were located in the ischiocondylar portion (3 in the proximal and 2 in the distal myoconnective junction) and 6 in the pubofemoral portion (4 in the distal and 2 in the proximal myoconnective junction). Most of the ischiocondylar lesions were myotendinous (3/5), and most of the pubofemoral lesions were myofascial (5/6). The BAMIC and MLG-R classification coincided in distinguishing injuries of moderate and mild severity. The management was nonoperative in all cases. The mean RTP time was 14 days (range, 0-35 days) and was longer in the ischiocondylar cases than in the pubofemoral cases (21 vs 8 days, respectively). Only 1 recurrence, at <10 months, was recorded.
Conclusion: Posteromedial thigh pain after an eccentric contraction during forced adduction of the thigh from hip internal rotation should raise a suspicion of AM lesions. The identification of the affected portion was possible on MRI. An injury in the ischiocondylar portion entailed a longer RTP time than an injury in the pubofemoral portion.
Keywords: BAMIC and MLG-R classification; MRI; adductor magnus injury; hip; pelvis; thigh.
© The Author(s) 2023.
Conflict of interest statement
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
Similar articles
-
Time to return to full training and recurrence of rectus femoris injuries in elite track and field athletes 2010-2019; a 9-year study using the British Athletics Muscle Injury Classification.Scand J Med Sci Sports. 2022 Jul;32(7):1109-1118. doi: 10.1111/sms.14160. Epub 2022 Mar 31. Scand J Med Sci Sports. 2022. PMID: 35332596
-
One-Year Clinical and Imaging Follow-up After Exercise-Based Treatment for Acute Complete Adductor Longus Tendon Avulsions in Athletes: A Prospective Case Series.Am J Sports Med. 2021 Sep;49(11):3004-3013. doi: 10.1177/03635465211015996. Epub 2021 Jun 23. Am J Sports Med. 2021. PMID: 34161743
-
Outcomes of Activity-Related Lower Extremity Muscle Tears After Application of the British Athletics Muscle Injury Classification: A Systematic Review.Sports Health. 2024 Sep-Oct;16(5):783-796. doi: 10.1177/19417381231195529. Epub 2023 Sep 8. Sports Health. 2024. PMID: 37681683 Free PMC article.
-
Application of the British Athletics Muscle Injury Classification in Collegiate Football Athletes: A Retrospective, Observational Study.Sports Health. 2025 Mar 27:19417381251326531. doi: 10.1177/19417381251326531. Online ahead of print. Sports Health. 2025. PMID: 40145663 Free PMC article.
-
Evidence-Based Management and Factors Associated With Return to Play After Acute Hamstring Injury in Athletes: A Systematic Review.Orthop J Sports Med. 2021 Nov 29;9(11):23259671211053833. doi: 10.1177/23259671211053833. eCollection 2021 Nov. Orthop J Sports Med. 2021. PMID: 34888392 Free PMC article. Review.
Cited by
-
Technique of Distal Tendon Excision for the Treatment of Chronic Pain Caused by Isolated Proximal Gracilis Tears.Arthrosc Tech. 2024 Jun 22;13(11):103099. doi: 10.1016/j.eats.2024.103099. eCollection 2024 Nov. Arthrosc Tech. 2024. PMID: 39711900 Free PMC article.
-
From Muscle to the Myofascial Unit: Current Evidence and Future Perspectives.Int J Mol Sci. 2023 Feb 24;24(5):4527. doi: 10.3390/ijms24054527. Int J Mol Sci. 2023. PMID: 36901958 Free PMC article. Review.
References
-
- Attarian DE. Isolated acute hip adductor brevis strain. J South Orthop Assoc. 2000;9(3):213–215. - PubMed
-
- Ballestero E, Duran C, Planas A, López Bedoya J, Vernetta M. Fuerza y dominancia lateral. Apunts Sports Med. 1997;1(47):74–80.
-
- Broski SM, Murthy NS, Krych AJ, Obey MR, Collins MS. The adductor magnus “mini-hamstring”: MRI appearance and potential pitfalls. Skeletal Radiol. 2016;45(2):213–219. - PubMed
-
- Chopra A, Robinson P. Imaging athletic groin pain. Radiol Clin North Am. 2016;54(5):865–873. - PubMed
-
- Delahunt E, Kennelly C, McEntee BL, Coughlan GF, Green BS. The thigh adductor squeeze test: 45° of hip flexion as the optimal test position for eliciting adductor muscle activity and maximum pressure values. Man Ther. 2011;16(5):476–480. - PubMed
LinkOut - more resources
Full Text Sources
