

Overt and Occult Hypoxemia in Patients Hospitalized With COVID-19
- PMID: 36699241
- PMCID: PMC9857543
- DOI: 10.1097/CCE.0000000000000825
Overt and Occult Hypoxemia in Patients Hospitalized With COVID-19
Abstract
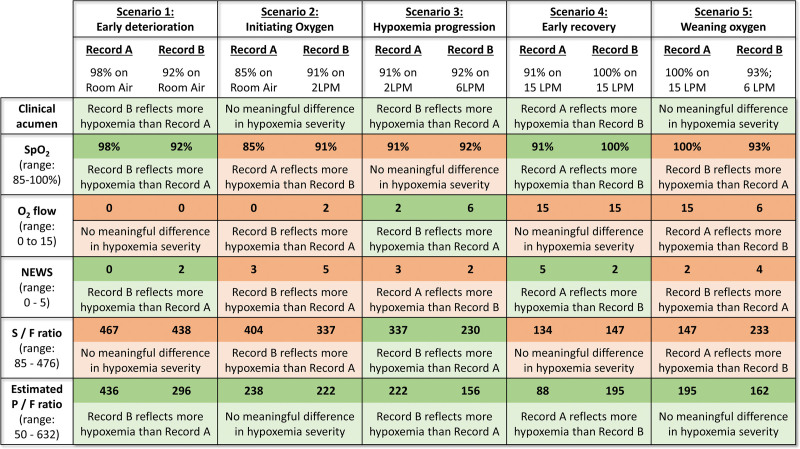
Progressive hypoxemia is the predominant mode of deterioration in COVID-19. Among hypoxemia measures, the ratio of the Pao2 to the Fio2 (P/F ratio) has optimal construct validity but poor availability because it requires arterial blood sampling. Pulse oximetry reports oxygenation continuously (ratio of the Spo2 to the Fio2 [S/F ratio]), but it is affected by skin color and occult hypoxemia can occur in Black patients. Oxygen dissociation curves allow noninvasive estimation of P/F ratios (ePFRs) but remain unproven.
Objectives: Measure overt and occult hypoxemia using ePFR.
Design setting and participants: We retrospectively studied COVID-19 hospital encounters (n = 5,319) at two academic centers (University of Virginia [UVA] and Emory University).
Main outcomes and measures: We measured primary outcomes (death or ICU transfer within 24 hr), ePFR, conventional hypoxemia measures, baseline predictors (age, sex, race, comorbidity), and acute predictors (National Early Warning Score [NEWS] and Sequential Organ Failure Assessment [SOFA]). We updated predictors every 15 minutes. We assessed predictive validity using adjusted odds ratios (AORs) and area under the receiver operating characteristic curves (AUROCs). We quantified disparities (Black vs non-Black) in empirical cumulative distributions using the Kolmogorov-Smirnov (K-S) two-sample test.
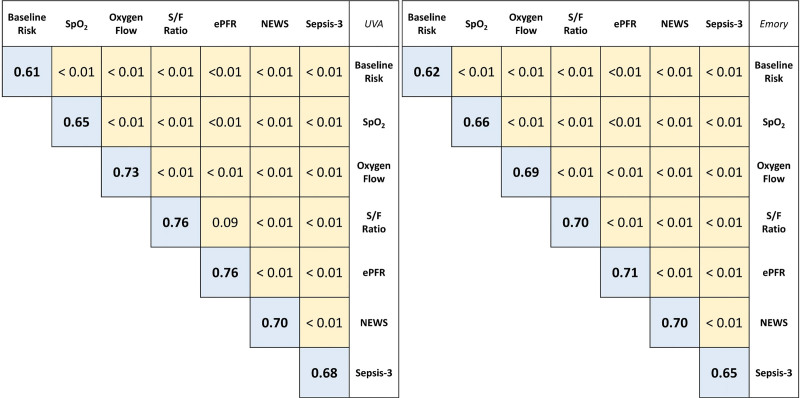
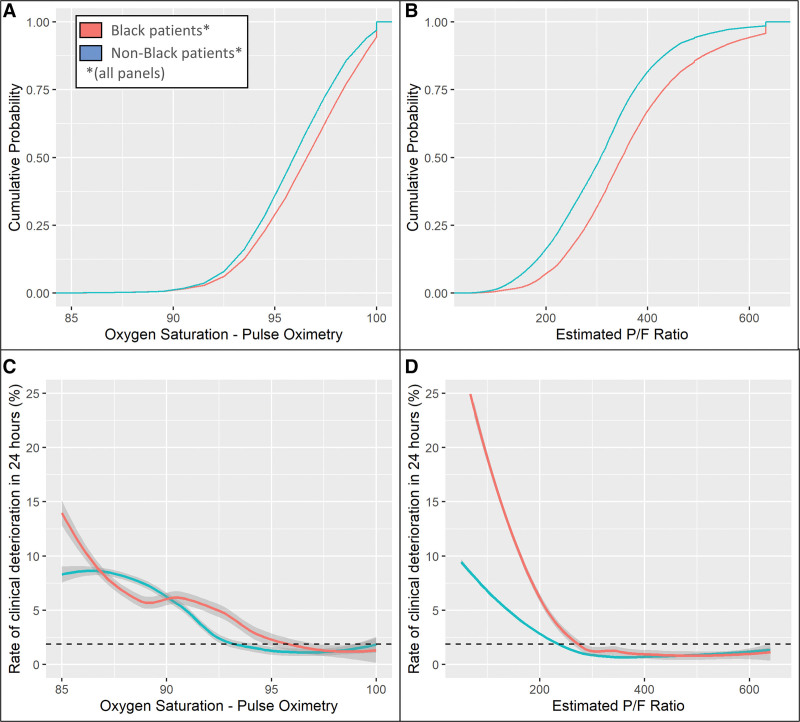
Results: Overt hypoxemia (low ePFR) predicted bad outcomes (AOR for a 100-point ePFR drop: 2.7 [UVA]; 1.7 [Emory]; p < 0.01) with better discrimination (AUROC: 0.76 [UVA]; 0.71 [Emory]) than NEWS (0.70 [both sites]) or SOFA (0.68 [UVA]; 0.65 [Emory]) and similar to S/F ratio (0.76 [UVA]; 0.70 [Emory]). We found racial differences consistent with occult hypoxemia. Black patients had better apparent oxygenation (K-S distance: 0.17 [both sites]; p < 0.01) but, for comparable ePFRs, worse outcomes than other patients (AOR: 2.2 [UVA]; 1.2 [Emory]; p < 0.01).
Conclusions and relevance: The ePFR was a valid measure of overt hypoxemia. In COVID-19, it may outperform multi-organ dysfunction models. By accounting for biased oximetry as well as clinicians' real-time responses to it (supplemental oxygen adjustment), ePFRs may reveal racial disparities attributable to occult hypoxemia.
Keywords: COVID-19; hospital mortality; organ dysfunction scores; prognosis; respiratory failure.
Copyright © 2023 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
Dr. Moore is supported by the National Institutes of Health (U01AI150508). Dr. Holder is supported by the National Institutes of Health (K23GM37182), and he has received speaker and consulting fees from Baxter International and Philips, respectively. Dr. Kamaleswaran was supported by the National Institutes of Health (R01GM139967). Dr. Clark is an employee of Nihon Kohden Digital Health Solutions (Irvine, CA). Dr. Moorman has equity in Medical Predictive Science Corporation, Charlottesville, VA, and consults for Nihon Kohden Digital Health Solutions, Irvine, CA, with proceeds donated to the University of Virginia Medical Foundation. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Update of
-
Overt and occult hypoxemia in patients hospitalized with novel coronavirus disease 2019.medRxiv [Preprint]. 2022 Jun 16:2022.06.14.22276166. doi: 10.1101/2022.06.14.22276166. medRxiv. 2022. Update in: Crit Care Explor. 2023 Jan 20;5(1):e0825. doi: 10.1097/CCE.0000000000000825. PMID: 35734082 Free PMC article. Updated. Preprint.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
