

Impact of Antibiotic Time-Outs in Multidisciplinary ICU Rounds for Antimicrobial Stewardship Program on Patient Survival: A Controlled Before-and-After Study
- PMID: 36699244
- PMCID: PMC9829256
- DOI: 10.1097/CCE.0000000000000837
Impact of Antibiotic Time-Outs in Multidisciplinary ICU Rounds for Antimicrobial Stewardship Program on Patient Survival: A Controlled Before-and-After Study
Abstract
The antimicrobial stewardship program (ASP) is an important quality improvement initiative that is recommended in the ICU. However, the shortage of infectious disease physicians in Japan has led to the need for simpler methods for implementing ASPs. We investigated whether antibiotic time-outs (ATOs) during multidisciplinary rounds as part of an ASP can improve patient survival and reduce the number of days of therapy (DOT) with antibiotics.
Design: Single-center controlled before-and-after study.
Setting: Medical/surgical ICU in a tertiary university medical center in Tokyo, Japan.
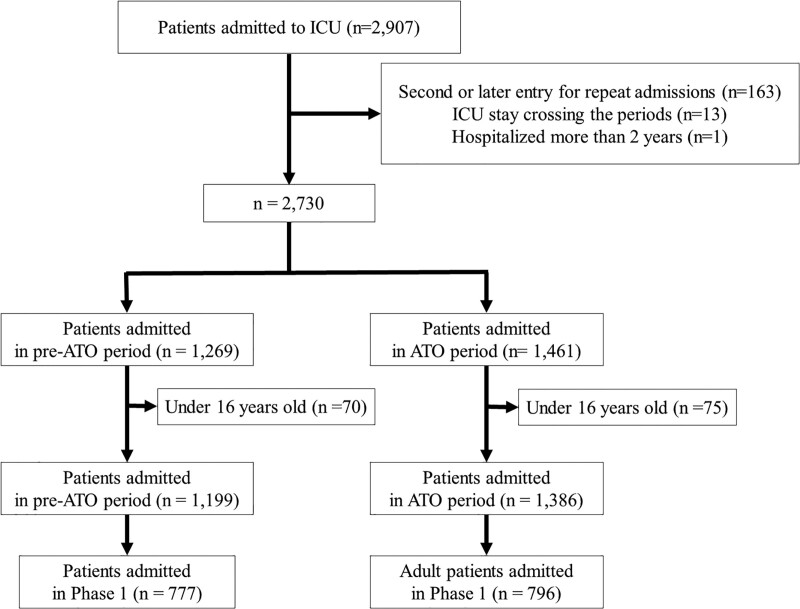
Patients: All patients 16 years old or older admitted consecutively in the ICU between October 2016 and March 2020.
Interventions: An intensivist-driven ICU multidisciplinary round was introduced in October 2016, and ATOs with ICU rounds were implemented in June 2018. ATOs were conducted 3, 7, and 14 days after initiation of antibiotics.
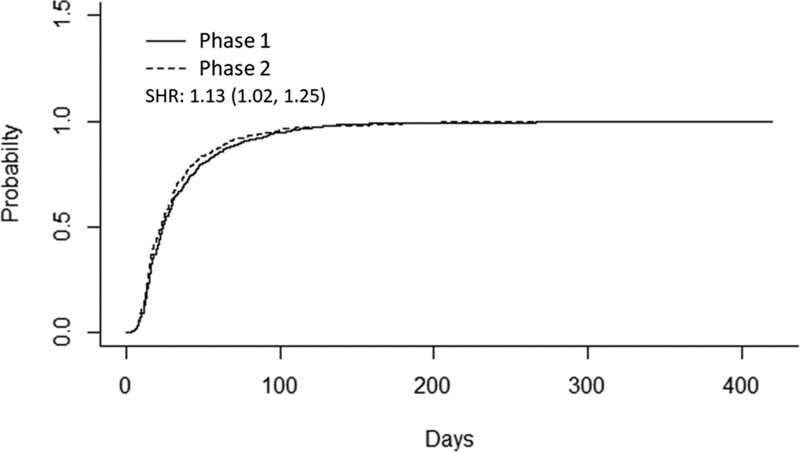
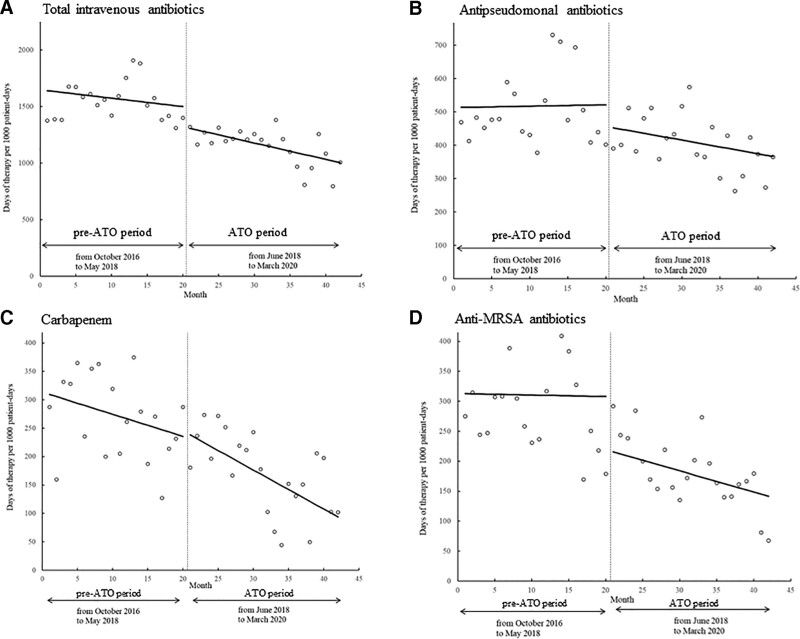
Measurements and main results: The primary outcome was the subdistribution hazard ratio (SHR) of survival to hospital discharge compared between multidisciplinary rounds (phase 1) and ATO during multidisciplinary rounds (phase 2) using the multivariable Fine-Gray model. The secondary outcomes were the SHR of survival to ICU discharge and the trends in the DOT with IV antibiotics per 1,000 patient-days between October 2016 and March 2020 by using interrupted time-series analysis. The number of patients in phases 1 and 2 was 777 and 796, respectively. The group that underwent ATO during multidisciplinary rounds showed a significant increase in the survival to hospital discharge in comparison with the multidisciplinary round-only group (SHR, 1.13; 95% CI, 1.02-1.25); however, the SHR of survival to ICU discharge showed no significant intergroup difference. The DOT with total IV antibiotics decreased after ATO implementation (change in intercept, -178.26; 95% CI, -317.74 to -38.78; change in slope, -7.00; 95% CI, -15.77 to 1.78).
Conclusions: ATOs during multidisciplinary rounds are associated with improved patient survival and reduced DOT.
Keywords: antibiotic time-out; antimicrobial stewardship program; intensive care unit; multidisciplinary rounds.
Copyright © 2023 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures
Similar articles
-
Cluster randomized trial of an antibiotic time-out led by a team-based pharmacist.Infect Control Hosp Epidemiol. 2020 Nov;41(11):1266-1271. doi: 10.1017/ice.2020.347. Epub 2020 Aug 20. Infect Control Hosp Epidemiol. 2020. PMID: 32814610 Clinical Trial.
-
Effect of discontinuation of an antimicrobial stewardship programme on the antibiotic usage pattern.Clin Microbiol Infect. 2021 Dec;27(12):1860.e1-1860.e5. doi: 10.1016/j.cmi.2021.07.019. Epub 2021 Jul 27. Clin Microbiol Infect. 2021. PMID: 34325066
-
Surgical intensive care - current and future challenges?Qatar Med J. 2020 Jan 13;2019(2):3. doi: 10.5339/qmj.2019.qccc.3. eCollection 2019. Qatar Med J. 2020. PMID: 31976309 Free PMC article.
-
[Antimicrobial stewardship program in an Intensive Care Unit: A retrospective observational analysis of the results 15 months after its implementation].Rev Esp Quimioter. 2023 Oct;36(5):477-485. doi: 10.37201/req/142.2022. Epub 2023 May 31. Rev Esp Quimioter. 2023. PMID: 37253230 Free PMC article. Spanish.
-
Antimicrobial Stewardship and Intensive Care Unit Mortality: A Systematic Review.Clin Infect Dis. 2019 Feb 15;68(5):748-756. doi: 10.1093/cid/ciy550. Clin Infect Dis. 2019. PMID: 29982376
Cited by
-
Lab efficiency and improvements in the management of bloodstream infections: a before and after study.Eur J Clin Microbiol Infect Dis. 2025 Jul 11. doi: 10.1007/s10096-025-05200-x. Online ahead of print. Eur J Clin Microbiol Infect Dis. 2025. PMID: 40643849 No abstract available.
References
-
- World Health Organization: Global Action Plan on Antimicrobial Resistance. 2016.. Available at: https://www.who.int/publications/i/item/9789241509763. Accessed February 10, 2022 - PubMed
LinkOut - more resources
Full Text Sources
