

Dyspnea in pregnancy might be related to the incomplete physiological adaptation of the heart
- PMID: 36699561
- PMCID: PMC9871158
- DOI: 10.34172/jcvtr.2022.30539
Dyspnea in pregnancy might be related to the incomplete physiological adaptation of the heart
Abstract
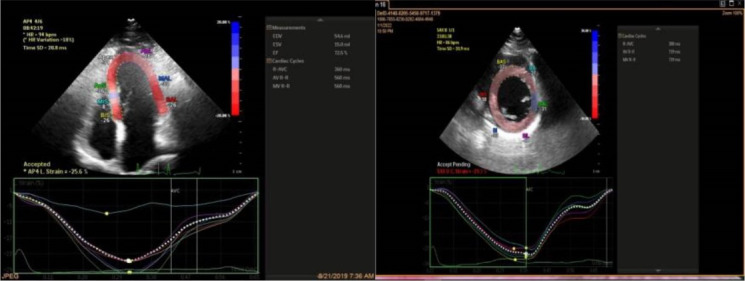
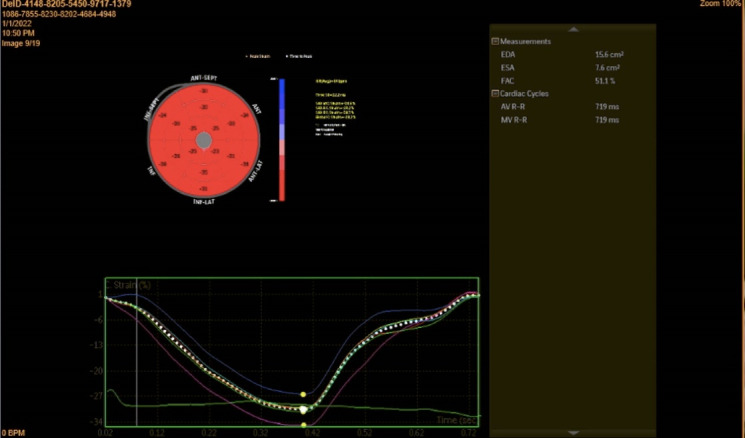
Introduction: Dyspnea is a common complaint in pregnant women with no cardiac and pulmonary diseases. We aimed to assess whether physiological dyspnea of pregnancy was correlated with subtle changes in ventricular systolic and diastolic function. Methods: This cross-sectional study enrolled 40 healthy pregnant women in their second and third trimesters with no complaints of dyspnea and 40 healthy pregnant women in the same trimesters with a complaint of dyspnea. Parameters of echocardiography were compared between the 2 groups. Results: Global left ventricular ejection fraction (59.65±6.44 and 58.49±4.95 P=0.418 in patients without and with dyspnea respectively), and global longitudinal strain were not significantly different (18.72±2.90 and 18.94±3.07, P=0.57 in the same order). Global circumferential strain (GCS) was lower in patients with dyspnea. (20.19±4.86 vs 22.61±4.69, P=0.03). Systolic volume (33.17±8.94 vs 32.63±8.09) and diastolic volume (80.75±18.73 vs 78.37±16.63) and left ventricular end-diastolic diameter (47.5±4.24 vs 46.23±3.21) were not different (P=0.784, 0.560 and 0.146 respectively). Left ventricular end-systolic diameter was significantly lower in the case group (32.52±4.66 vs 29.92±4.05, P=0.011). Left atrial area index in the patients with dyspnea was lower(8.13±1.42 vs 8.94±1.4, P=0.014). Other findings were a high E/E' and high pulmonary artery pressure in the patients with dyspnea. Conclusion: Dyspnea in pregnant women can be a consequence of incomplete physiological adaptation to volume overload in pregnancy. Lower systolic and diastolic diameters of the left ventricle, left atrial area, and left atrial index may lead to increased filling pressure, manifested by a higher E/E' ratio and pulmonary artery pressure.
Keywords: Dyspnea; Physiologic; Pregnancy; Shortness of Breath.
© 2022 The Author(s).
Similar articles
-
Changes in left ventricular and atrial mechanics and function after dialysis in patients with end-stage renal disease.Quant Imaging Med Surg. 2021 May;11(5):1899-1908. doi: 10.21037/qims-20-961. Quant Imaging Med Surg. 2021. PMID: 33936973 Free PMC article.
-
High frequency of diastolic dysfunction in a population-based cohort of elderly women--but poor association with the symptom dyspnea.BMC Geriatr. 2011 Nov 2;11:71. doi: 10.1186/1471-2318-11-71. BMC Geriatr. 2011. PMID: 22047619 Free PMC article.
-
Correlation of Left Atrial Strain and Doppler Measurements with Invasive Measurement of Left Ventricular End-Diastolic Pressure in Patients Stratified for Different Values of Ejection Fraction.Echocardiography. 2016 Mar;33(3):398-405. doi: 10.1111/echo.13094. Epub 2015 Oct 23. Echocardiography. 2016. PMID: 26493278
-
Longitudinal, circumferential and radial systolic left ventricular function in patients with heart failure and preserved ejection fraction.Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2016 Sep;160(3):385-92. doi: 10.5507/bp.2016.007. Epub 2016 Mar 4. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2016. PMID: 26948032
-
[Effect of positive end-expiratory pressure on cardiac function in patients with early left ventricular diastolic dysfunction: a prospective cohort study].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2022 Oct;34(10):1066-1071. doi: 10.3760/cma.j.cn121430-20220414-00369. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2022. PMID: 36473565 Chinese.
References
LinkOut - more resources
Full Text Sources