

Pre-operative predictive factors of residual varus on the mechanical axis after Oxford unicompartmental knee arthroplasty
- PMID: 36700020
- PMCID: PMC9869032
- DOI: 10.3389/fsurg.2022.1054351
Pre-operative predictive factors of residual varus on the mechanical axis after Oxford unicompartmental knee arthroplasty
Abstract
Background: Residual varus after Oxford unicompartmental knee arthroplasty (UKA) happens frequently. This study aims to evaluate the pre-operative contributing factors of residual varus.
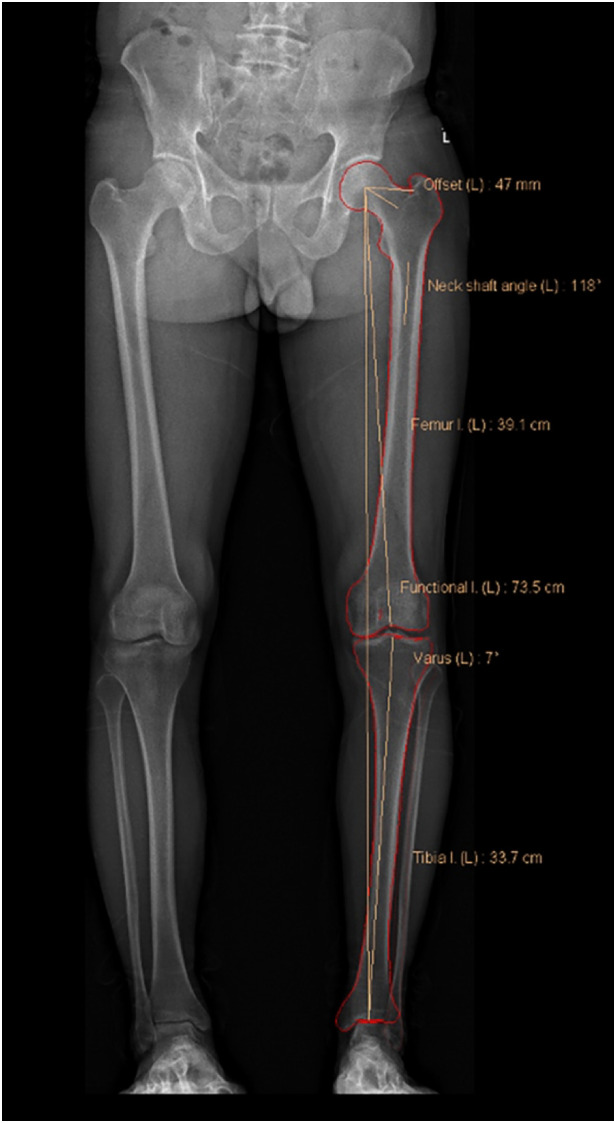
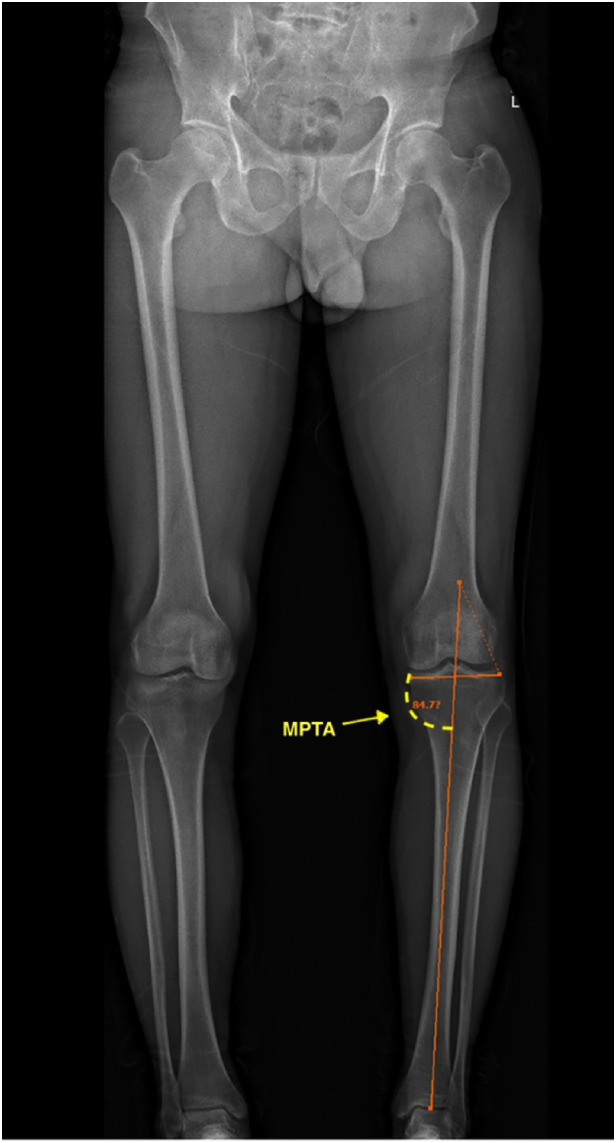
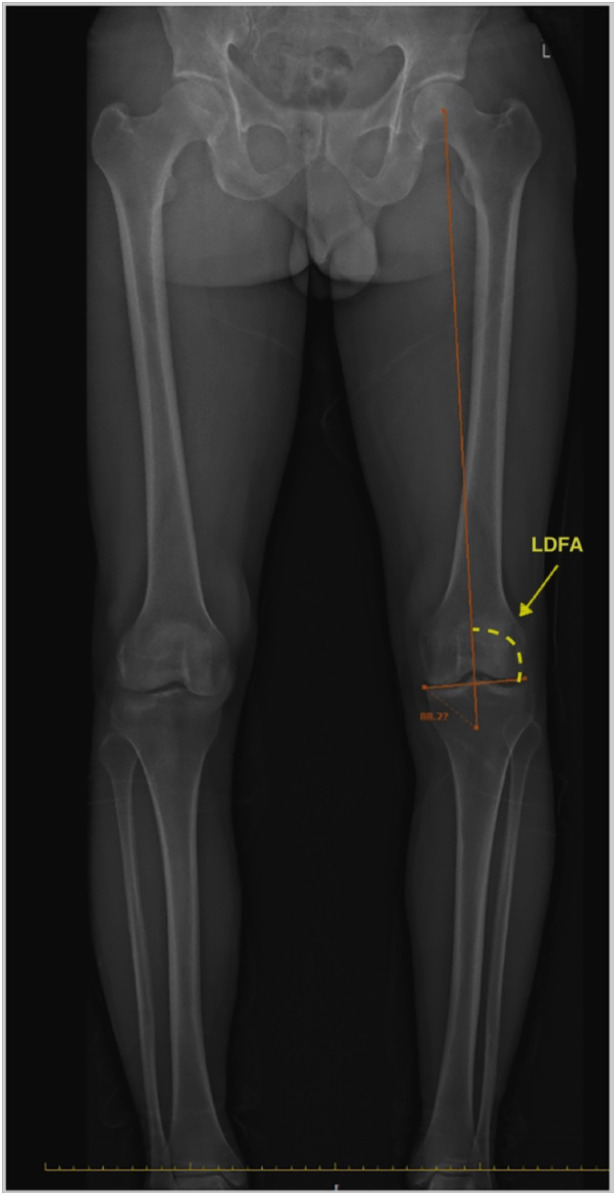
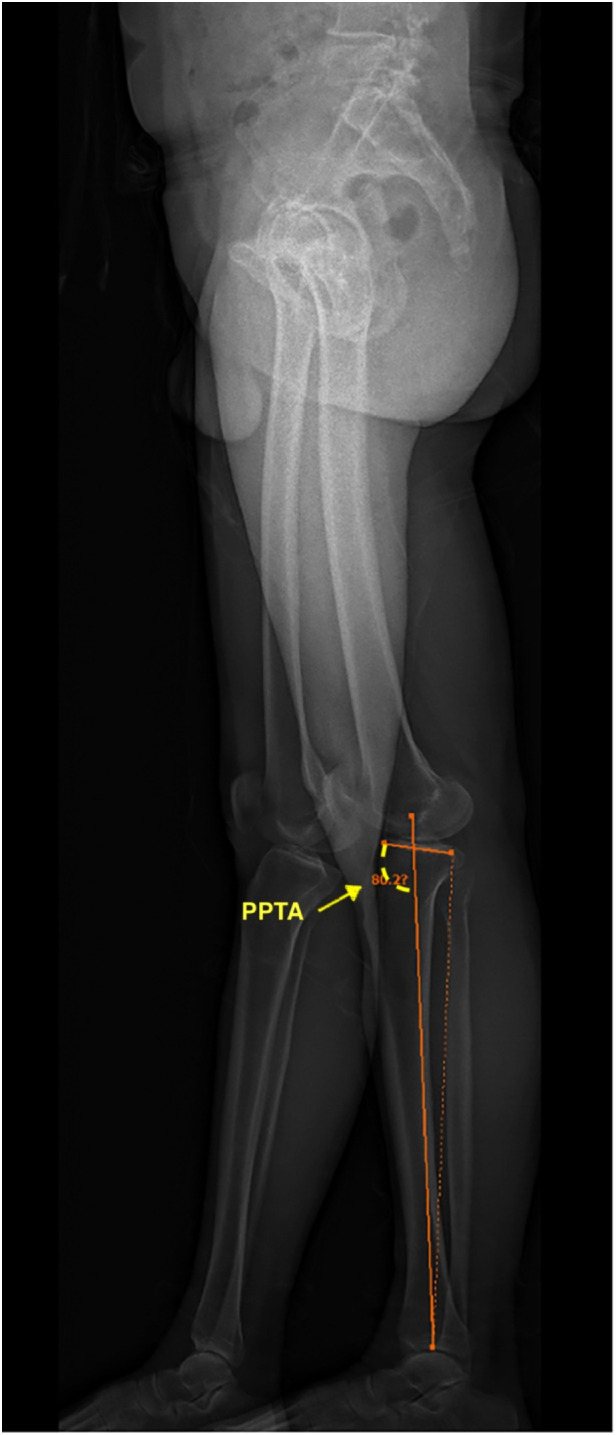
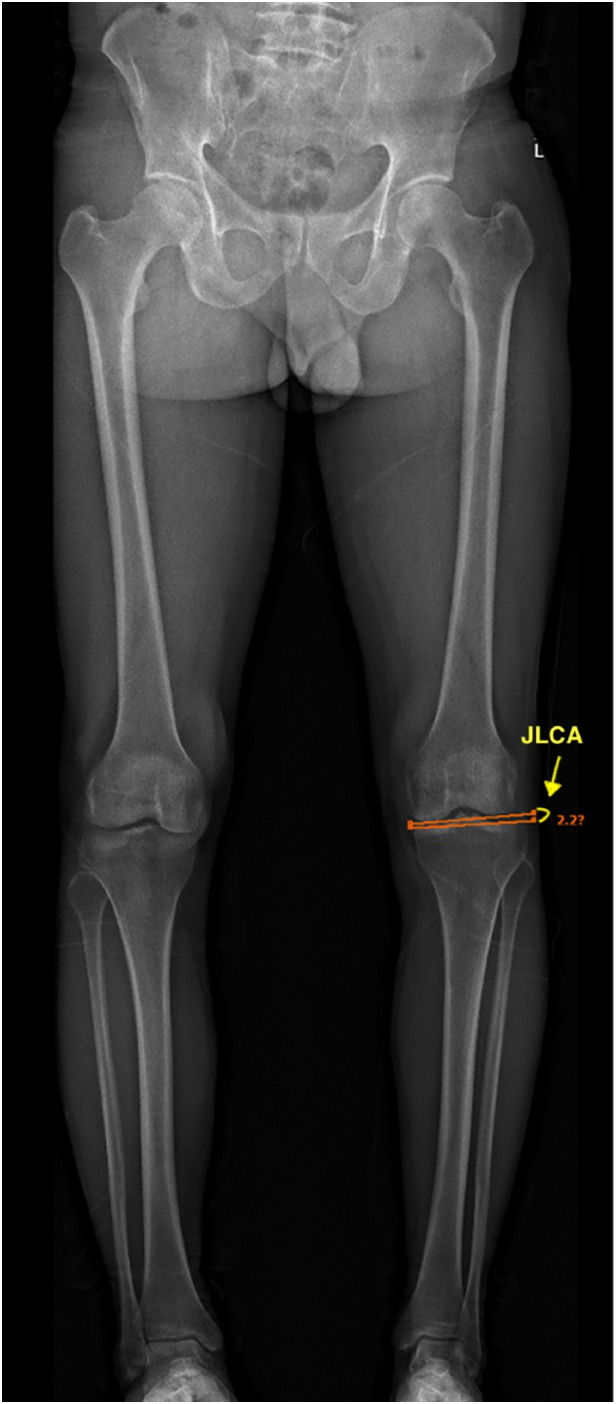
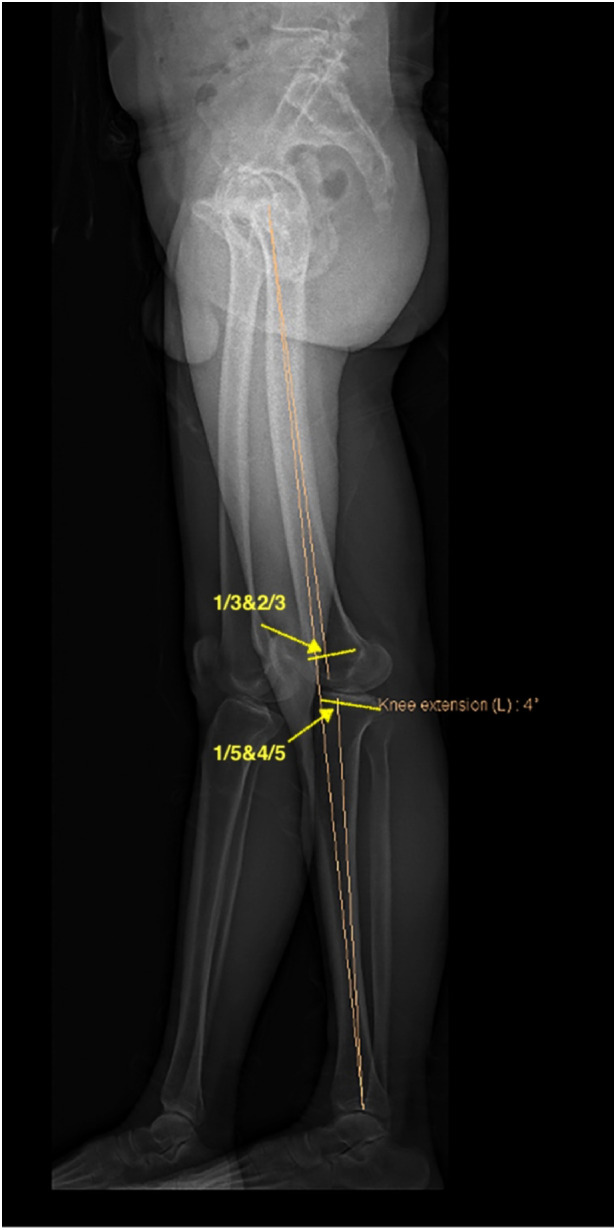
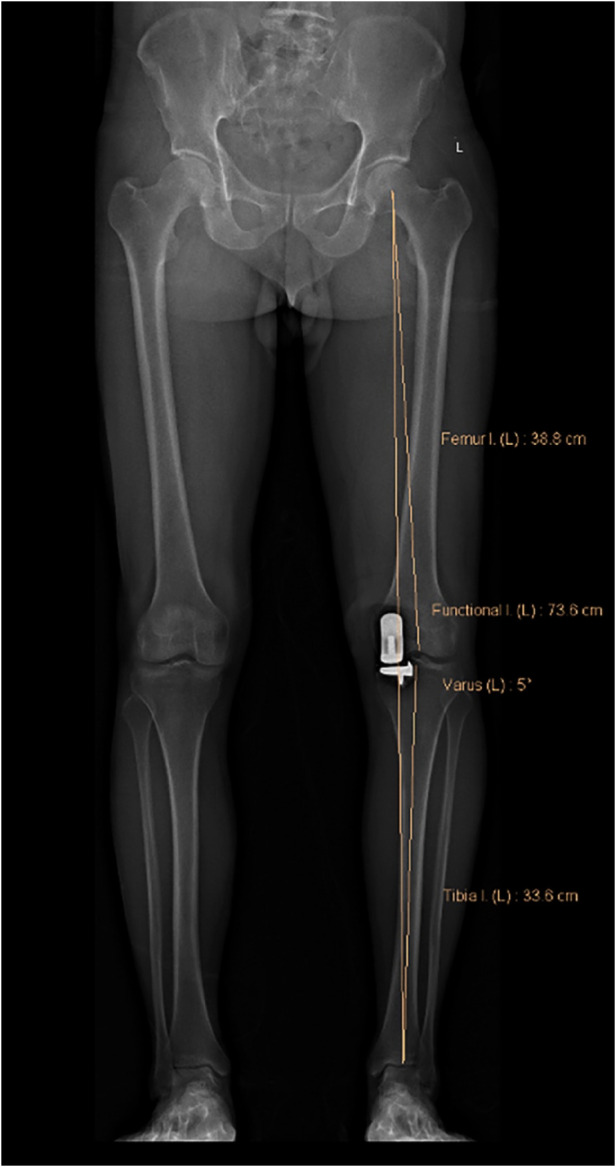
Methods: A total of 1,002 knees (880 patients, 201 patients were male, and 679 were female) underwent Oxford UKA in the Orthopedic Surgery Department of the Beijing Jishuitan Hospital from March 2018 to April 2021. The mean age of the patient was 64.7 ± 7.7 years. To assess residual varus, the full-length lower extremity is placed upright for EOS imaging, with the knee fully extended. The angle of post-operative residual varus was measured as described by Noyes et al. Of the knees studied, they were either categorized into an under-corrected group (post-operative Noyes angle >5°) or a corrected group (post-operative Noyes angle ≤5°). Age, gender, body mass index (BMI), range of motion (ROM), Clinical American Knee Society Score (Clinical AKSS), and Function American Knee Society Score (Function AKSS) were compared. The following additional parameters were measured: pre-operative Noyes angle, lateral distal femoral angle (LDFA), medial proximal tibial angle (MPTA), the posterior slope of the proximal tibia angle (PPTA), joint line converge angle (JLCA), and fixed flexion deformity (FFD).
Results: There was no statistically significant difference between the two groups in regards to gender (p = 0.428), surgical leg (p = 0.937), age (p = 0.851), BMI (p = 0.064), pre-operative Clinical AKSS (p = 0.206) and Function AKSS (p = 0.100). However, pre-operative ROM statistically differed between the two groups (p < 0.001). The contributing factors of post-operative residual varus were determined to be the following parameters: pre-operative MPTA (p < 0.001, OR = 4.522, 95% CI: 2.927-6.984), pre-operative Noyes (p < 0.001, OR = 3.262, 95% CI: 1.802-5.907) and pre-operative FFD (p = 0.007, OR = 1.862, 95% CI: 1.182-2.934). The effects of pre-operative LDFA (p = 0.146), JLCA (p = 0.942), and pre-operative PPTA (p = 0.899) on the post-operative mechanical axis did not show statistical significance.
Conclusions: Patients with severe pre-operative varus, particularly varus deformity mainly from the tibial side or pre-operative FFD, are more prone to get extremity mechanical axis residual varus after UKA with Oxford.
Keywords: biplanar radiograph; lower limb alignment; moblie-bearing; predictor; unicompartemtal knee arthroplasty.
© 2023 Ji, Huang, Zhou, Wang, Wang, Ma and Jiang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Multivariate analysis of varus after Oxford unicompartmental knee arthroplasty].Beijing Da Xue Xue Bao Yi Xue Ban. 2021 Mar 11;53(2):293-297. doi: 10.19723/j.issn.1671-167X.2021.02.010. Beijing Da Xue Xue Bao Yi Xue Ban. 2021. PMID: 33879900 Free PMC article. Chinese.
-
Asymmetric transepicondylar axis between varus and valgus osteoarthritic knees in windswept deformity can be predicted by hip-knee-ankle angle difference.Knee Surg Sports Traumatol Arthrosc. 2022 Sep;30(9):3024-3031. doi: 10.1007/s00167-021-06661-1. Epub 2021 Jul 14. Knee Surg Sports Traumatol Arthrosc. 2022. PMID: 34258661
-
A residual intra-articular varus after medial opening wedge high tibial osteotomy (HTO) for varus osteoarthritis of the knee.Arch Orthop Trauma Surg. 2019 Jun;139(6):743-750. doi: 10.1007/s00402-018-03104-4. Epub 2019 Jan 23. Arch Orthop Trauma Surg. 2019. PMID: 30673869
-
Risk factors of post-operative malalignment in fixed-bearing medial unicompartmental knee arthroplasty.Int Orthop. 2016 Jul;40(7):1455-63. doi: 10.1007/s00264-015-3014-1. Epub 2015 Oct 10. Int Orthop. 2016. PMID: 26452679
-
A flat all-polyethylene tibial component in medial unicompartmental knee arthroplasty: a long-term study.Knee. 2014;21 Suppl 1:S20-5. doi: 10.1016/S0968-0160(14)50005-1. Knee. 2014. PMID: 25382363 Review.
Cited by
-
High tibial lateral closing wedge and opening wedge valgus osteotomy produce different effects on posterior tibial slope and patellar height.Front Surg. 2023 Sep 12;10:1219614. doi: 10.3389/fsurg.2023.1219614. eCollection 2023. Front Surg. 2023. PMID: 37780911 Free PMC article.
References
-
- Lim JBT, Pang HN, Tay KJD, Chia SL, Lo NN, Yeo SJ. Clinical outcomes and patient satisfaction following revision of failed unicompartmental knee arthroplasty to total knee arthroplasty are as good as a primary total knee arthroplasty. Knee. (2019) 26:847–52. 10.1016/j.knee.2019.04.016 - DOI - PubMed
-
- Casper DS, Fleischman AN, Papas PV, Grossman J, Scuderi GR, Lonner JH. Unicompartmental knee arthroplasty provides significantly greater improvement in function than total knee arthroplasty despite equivalent satisfaction for isolated medial compartment osteoarthritis. J Arthroplasty. (2019) 34:1611–6. 10.1016/j.arth.2019.04.005 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous