

Treatment of De Novo Renal Transplant Recipients With Calcineurin Inhibitor-free, Belatacept Plus Everolimus-based Immunosuppression
- PMID: 36700062
- PMCID: PMC9820789
- DOI: 10.1097/TXD.0000000000001419
Treatment of De Novo Renal Transplant Recipients With Calcineurin Inhibitor-free, Belatacept Plus Everolimus-based Immunosuppression
Abstract
Compared with calcineurin inhibitor-based immunosuppression, belatacept (BELA)-based treatment has been associated with better renal function but higher acute rejection rates. This phase 2 study (NCT02137239) compared the antirejection efficacy of BELA plus everolimus (EVL) with tacrolimus (TAC) plus mycophenolate mofetil (MMF), each following lymphocyte-depleting induction and rapid corticosteroid withdrawal.
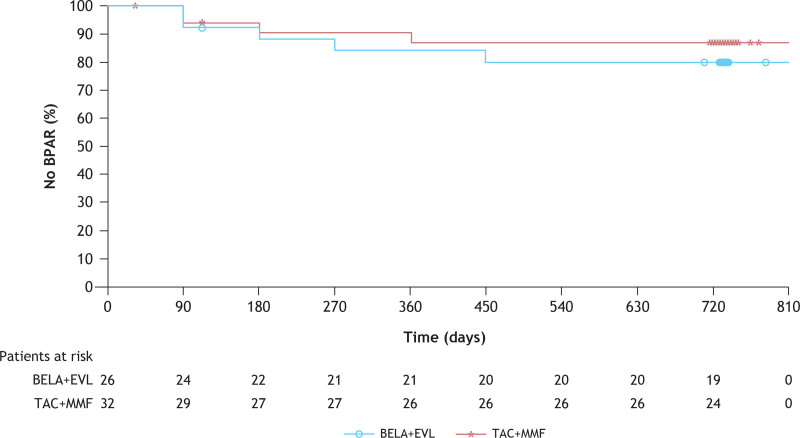
Methods: Patients who were de novo renal transplant recipients seropositive for Epstein-Barr virus were randomized to receive BELA+EVL or TAC+MMF maintenance therapy after rabbit antithymocyte globulin induction and up to 7 d of corticosteroids. The primary endpoint was the rate of biopsy-proven acute rejection at month 6.
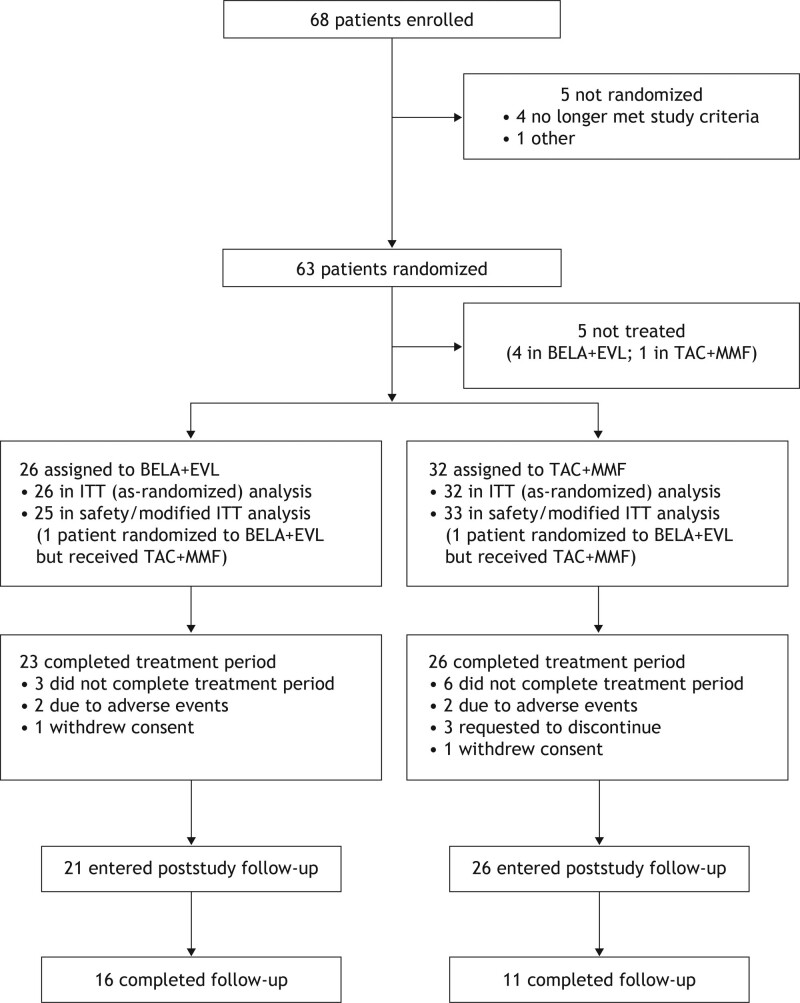
Results: Because of an unanticipated BELA supply constraint, enrollment was prematurely terminated at 68 patients, of whom 58 were randomized and transplanted (intention-to-treat [ITT] population: n = 26, BELA+EVL; n = 32, TAC+MMF). However, 25 patients received BELA+EVL' and 33 received TAC+MMF (modified ITT population). In the ITT population, the 6-mo biopsy-proven acute rejection rates were 7.7% versus 9.4% in the BELA+EVL versus TAC+MMF group. The corresponding 24-mo biopsy-proven acute rejection rates were 19.2% versus 12.5% in the ITT population and 16.0% versus 15.2% in the mITT population; all events were Banff severity grade ≤IIA and similar between groups. One patient in each group experienced graft loss unrelated to acute rejection. The 24-mo mean unadjusted estimated glomerular filtration rates were 71.8 versus 68.7 mL/min/1.73 m2 in the BELA+EVL versus TAC+MMF groups. Posttransplant lymphoproliferative disorder was reported for 1 patient in each group. No deaths or unexpected adverse events were observed.
Conclusions: A steroid-free maintenance regimen of BELA+EVL may be associated with biopsy-proven acute rejection rates comparable to TAC+MMF.
Copyright © 2023 The Author(s). Transplantation Direct. Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
V.R.P. has received consulting fees from CareDx and Transplant Genomics. J.O. has received consulting fees from Sigilon Therapeutics, has participated in the data safety and monitoring board for Sigilon Therapeutics and Avengebio, has a leadership/ fiduciary role in CellTrans Inc, and has stock/stock options in Sigilon Therapeutics and CellTrans Inc. L.A. is an employee of Bristol Myers Squibb. M.P. is an employee of and owns stock in Bristol Myers Squibb. R.N.F. has received consulting fees from Genentech, Novartis, Veloxis Pharmaceuticals, and Mallinckrodt Pharmaceuticals and has a leadership/fiduciary role at the American Society of Transplantation, OPTN/UNOS. The other authors declare no conflicts of interest.
Figures
References
-
- Azzi JR, Sayegh MH, Mallat SG. Calcineurin inhibitors: 40 years later, can’t live without. J Immunol. 2013;191:5785–5791. - PubMed
-
- Ekberg H. Calcineurin inhibitor sparing in renal transplantation. Transplantation. 2008;86:761–767. - PubMed
-
- Veenstra DL, Best JH, Hornberger J, et al. . Incidence and long-term cost of steroid-related side effects after renal transplantation. Am J Kidney Dis. 1999;33:829–839. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
