

Gestational age at birth and body size from infancy through adolescence: An individual participant data meta-analysis on 253,810 singletons in 16 birth cohort studies
- PMID: 36701266
- PMCID: PMC9879424
- DOI: 10.1371/journal.pmed.1004036
Gestational age at birth and body size from infancy through adolescence: An individual participant data meta-analysis on 253,810 singletons in 16 birth cohort studies
Erratum in
-
Correction: Gestational age at birth and body size from infancy through adolescence: An individual participant data meta-analysis on 253,810 singletons in 16 birth cohort studies.PLoS Med. 2023 Apr 18;20(4):e1004232. doi: 10.1371/journal.pmed.1004232. eCollection 2023 Apr. PLoS Med. 2023. PMID: 37071835 Free PMC article.
Abstract
Background: Preterm birth is the leading cause of perinatal morbidity and mortality and is associated with adverse developmental and long-term health outcomes, including several cardiometabolic risk factors and outcomes. However, evidence about the association of preterm birth with later body size derives mainly from studies using birth weight as a proxy of prematurity rather than an actual length of gestation. We investigated the association of gestational age (GA) at birth with body size from infancy through adolescence.
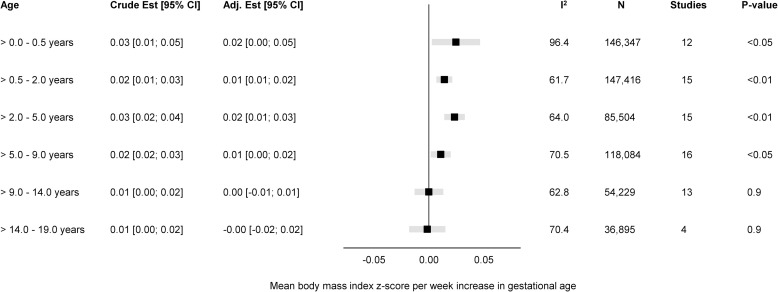
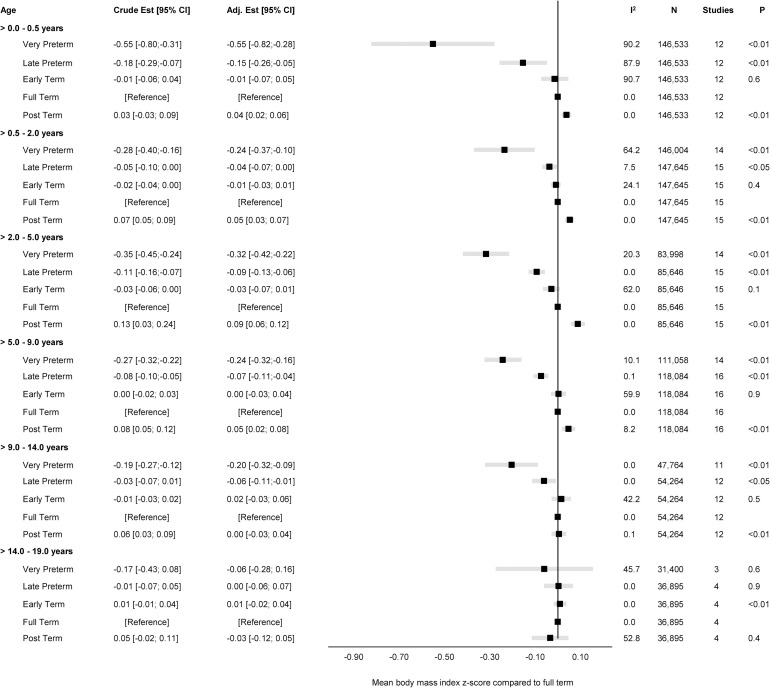
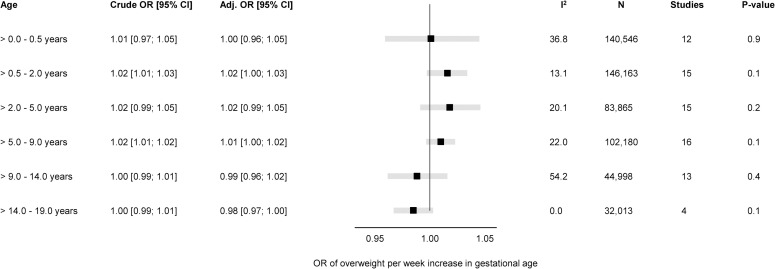
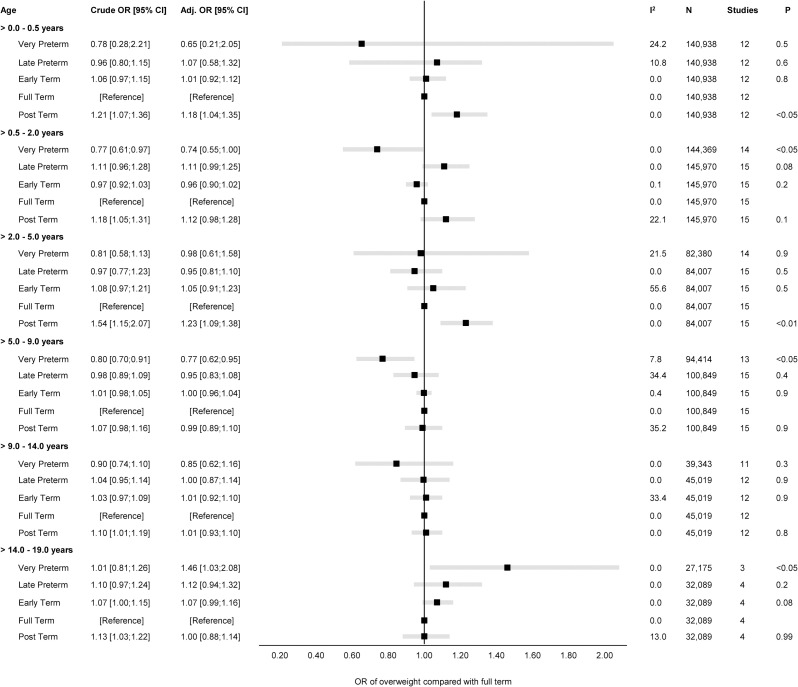
Methods and findings: We conducted a two-stage individual participant data (IPD) meta-analysis using data from 253,810 mother-child dyads from 16 general population-based cohort studies in Europe (Denmark, Finland, France, Italy, Norway, Portugal, Spain, the Netherlands, United Kingdom), North America (Canada), and Australasia (Australia) to estimate the association of GA with body mass index (BMI) and overweight (including obesity) adjusted for the following maternal characteristics as potential confounders: education, height, prepregnancy BMI, ethnic background, parity, smoking during pregnancy, age at child's birth, gestational diabetes and hypertension, and preeclampsia. Pregnancy and birth cohort studies from the LifeCycle and the EUCAN-Connect projects were invited and were eligible for inclusion if they had information on GA and minimum one measurement of BMI between infancy and adolescence. Using a federated analytical tool (DataSHIELD), we fitted linear and logistic regression models in each cohort separately with a complete-case approach and combined the regression estimates and standard errors through random-effects study-level meta-analysis providing an overall effect estimate at early infancy (>0.0 to 0.5 years), late infancy (>0.5 to 2.0 years), early childhood (>2.0 to 5.0 years), mid-childhood (>5.0 to 9.0 years), late childhood (>9.0 to 14.0 years), and adolescence (>14.0 to 19.0 years). GA was positively associated with BMI in the first decade of life, with the greatest increase in mean BMI z-score during early infancy (0.02, 95% confidence interval (CI): 0.00; 0.05, p < 0.05) per week of increase in GA, while in adolescence, preterm individuals reached similar levels of BMI (0.00, 95% CI: -0.01; 0.01, p 0.9) as term counterparts. The association between GA and overweight revealed a similar pattern of association with an increase in odds ratio (OR) of overweight from late infancy through mid-childhood (OR 1.01 to 1.02) per week increase in GA. By adolescence, however, GA was slightly negatively associated with the risk of overweight (OR 0.98 [95% CI: 0.97; 1.00], p 0.1) per week of increase in GA. Although based on only four cohorts (n = 32,089) that reached the age of adolescence, data suggest that individuals born very preterm may be at increased odds of overweight (OR 1.46 [95% CI: 1.03; 2.08], p < 0.05) compared with term counterparts. Findings were consistent across cohorts and sensitivity analyses despite considerable heterogeneity in cohort characteristics. However, residual confounding may be a limitation in this study, while findings may be less generalisable to settings in low- and middle-income countries.
Conclusions: This study based on data from infancy through adolescence from 16 cohort studies found that GA may be important for body size in infancy, but the strength of association attenuates consistently with age. By adolescence, preterm individuals have on average a similar mean BMI to peers born at term.
Copyright: © 2023 Vinther et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: DAL has received support from Roche Diagnostics and Medtronic in relation to biomarker research that is not related to the research presented in this paper. The other authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Grants and funding
- MC_PC_19009/MRC_/Medical Research Council/United Kingdom
- AA/18/7/34219/BHF_/British Heart Foundation/United Kingdom
- MR/S003959/2/MRC_/Medical Research Council/United Kingdom
- MC_PC_21038/MRC_/Medical Research Council/United Kingdom
- MC_PC_15018/MRC_/Medical Research Council/United Kingdom
- MC_UU_00011/6/MRC_/Medical Research Council/United Kingdom
- CH/F/20/90003/BHF_/British Heart Foundation/United Kingdom
- MR/N024397/1/MRC_/Medical Research Council/United Kingdom
- CS/16/4/32482/BHF_/British Heart Foundation/United Kingdom
- G9815508/MRC_/Medical Research Council/United Kingdom
- MR/S003959/1/MRC_/Medical Research Council/United Kingdom
