

Differential Diagnosis of Suspected Chronic Obstructive Pulmonary Disease Exacerbations in the Acute Care Setting: Best Practice
- PMID: 36701677
- PMCID: PMC10161746
- DOI: 10.1164/rccm.202209-1795CI
Differential Diagnosis of Suspected Chronic Obstructive Pulmonary Disease Exacerbations in the Acute Care Setting: Best Practice
Abstract
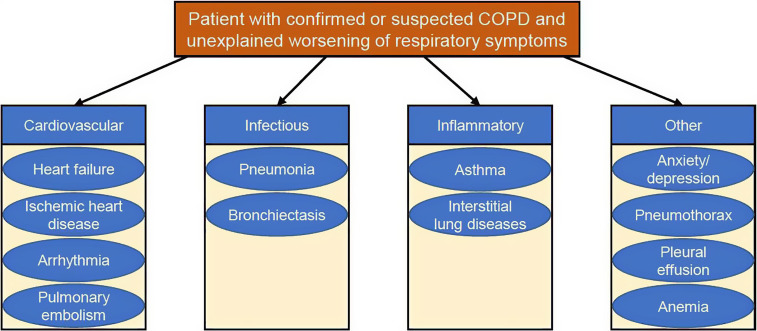
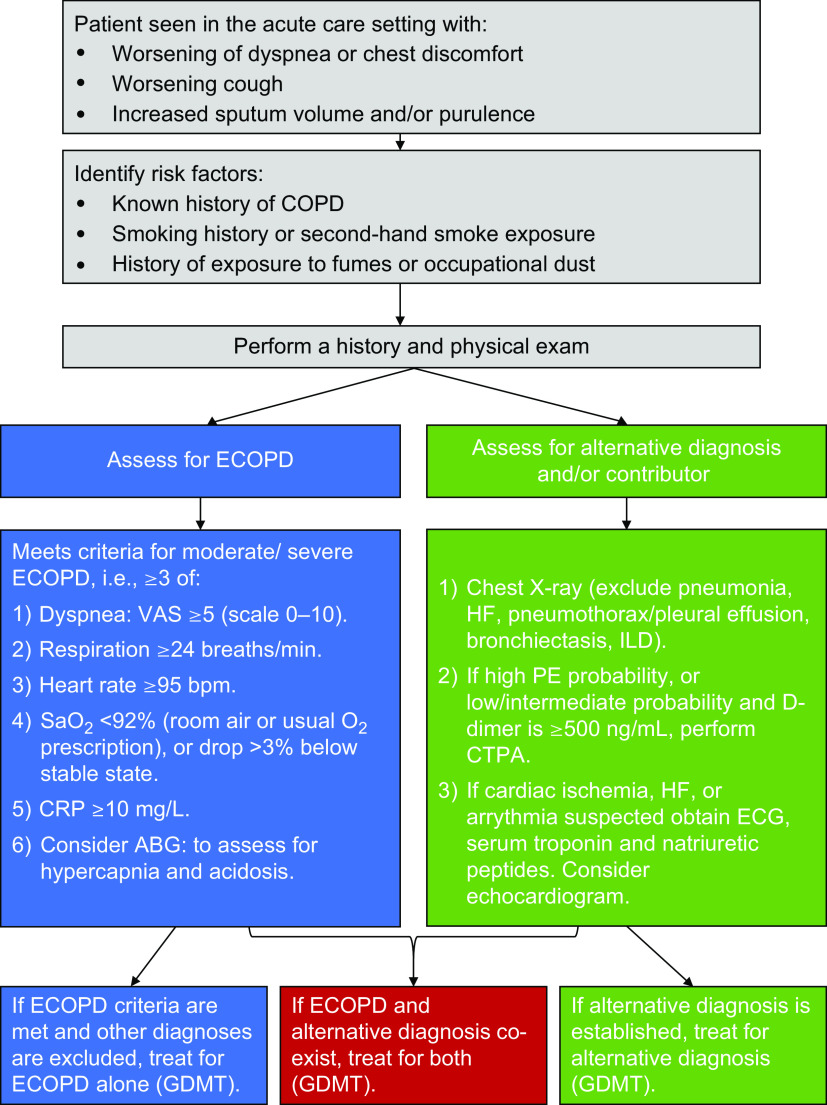
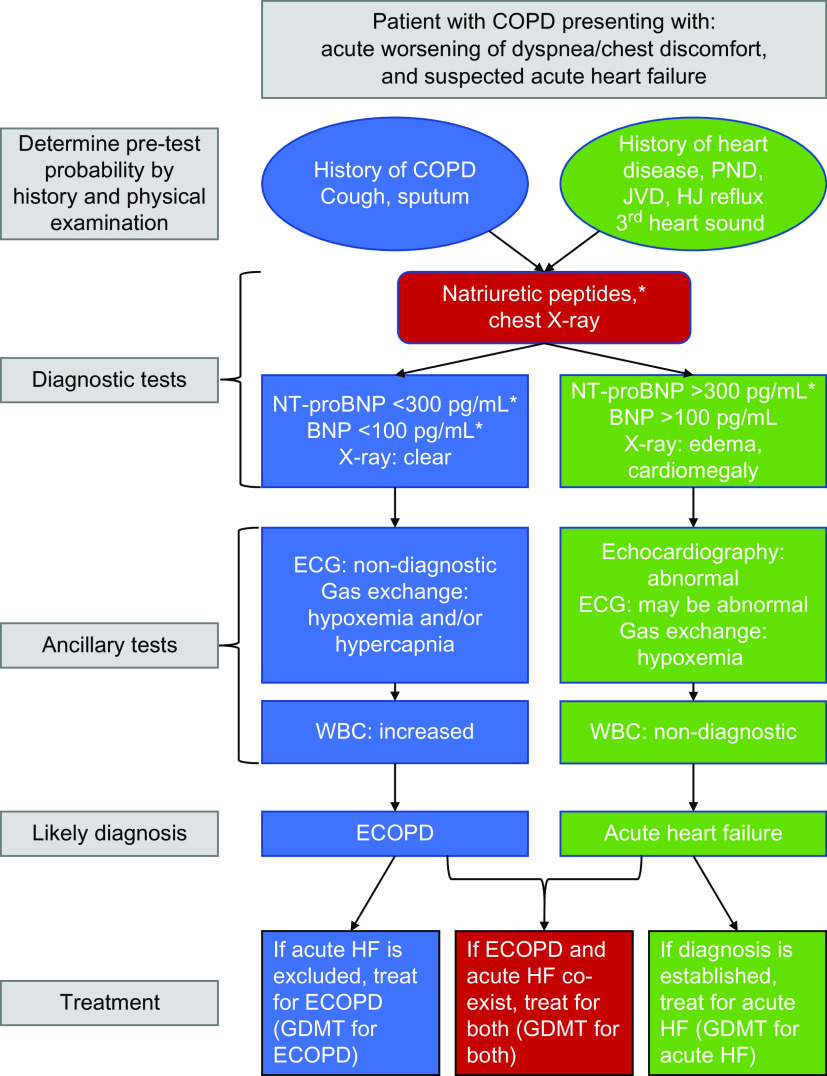
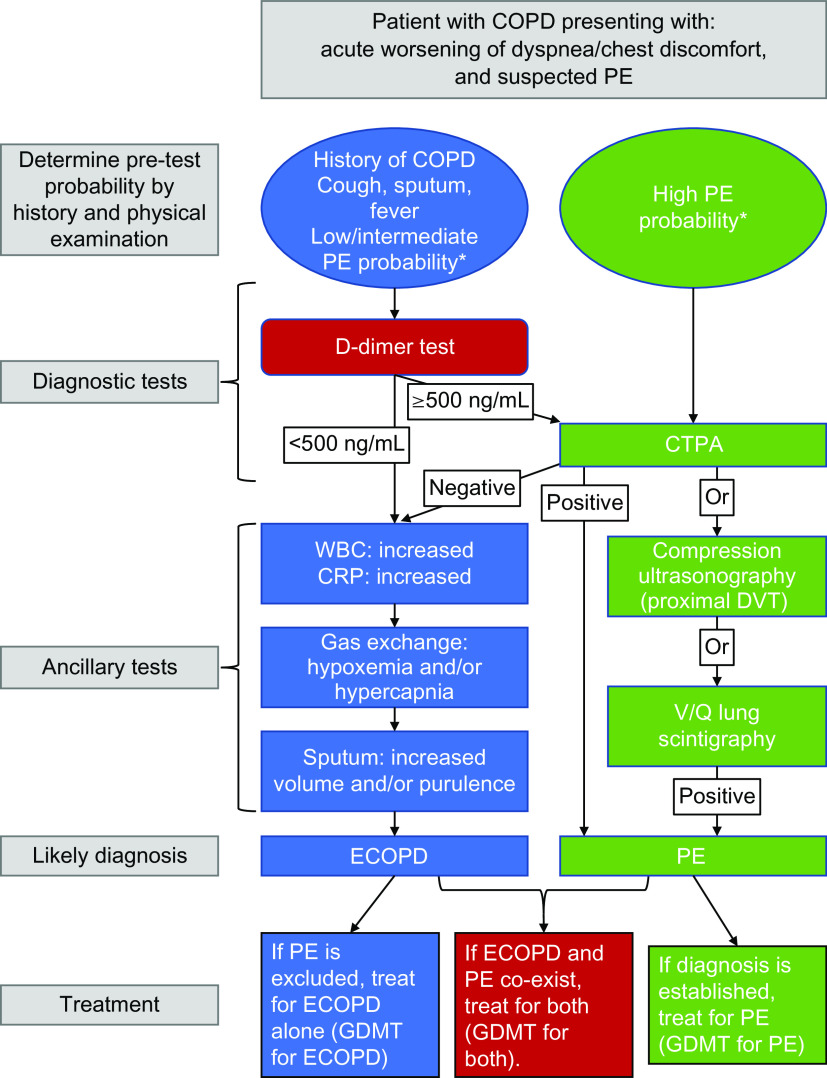
Patients with chronic obstructive pulmonary disease (COPD) may suffer from acute episodes of worsening dyspnea, often associated with increased cough, sputum, and/or sputum purulence. These exacerbations of COPD (ECOPDs) impact health status, accelerate lung function decline, and increase the risk of hospitalization. Importantly, close to 20% of patients are readmitted within 30 days after hospital discharge, with great cost to the person and society. Approximately 25% and 65% of patients hospitalized for an ECOPD die within 1 and 5 years, respectively. Patients with COPD are usually older and frequently have concomitant chronic diseases, including heart failure, coronary artery disease, arrhythmias, interstitial lung diseases, bronchiectasis, asthma, anxiety, and depression, and are also at increased risk of developing pneumonia, pulmonary embolism, and pneumothorax. All of these morbidities not only increase the risk of subsequent ECOPDs but can also mimic or aggravate them. Importantly, close to 70% of readmissions after an ECOPD hospitalization result from decompensation of other morbidities. These observations suggest that in patients with COPD with worsening dyspnea but without the other classic characteristics of ECOPD, a careful search for these morbidities can help detect them and allow appropriate treatment. For most morbidities, a thorough clinical evaluation supplemented by appropriate clinical investigations can guide the healthcare provider to make a precise diagnosis. This perspective integrates the currently dispersed information available and provides a practical approach to patients with COPD complaining of worsening respiratory symptoms, particularly dyspnea. A systematic approach should help improve outcomes and the personal and societal cost of ECOPDs.
Keywords: COPD; algorithms; differential diagnosis; symptom flare-up.
Figures
References
-
- Global Initiative for Chronic Obstructive Lung Disease. 2023. https://goldcopd.org/2023-gold-report-2/
-
- Riley CM, Sciurba FC. Diagnosis and outpatient management of chronic obstructive pulmonary disease: a review. JAMA . 2019;321:786–797. - PubMed
-
- Celli BR, Wedzicha JA. Update on clinical aspects of chronic obstructive pulmonary disease. N Engl J Med . 2019;381:1257–1266. - PubMed
-
- Divo M, Cote C, de Torres JP, Casanova C, Marin JM, Pinto-Plata V, et al. BODE Collaborative Group Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med . 2012;186:155–161. - PubMed
-
- MacLeod M, Papi A, Contoli M, Beghé B, Celli BR, Wedzicha JA, et al. Chronic obstructive pulmonary disease exacerbation fundamentals: diagnosis, treatment, prevention and disease impact. Respirology . 2021;26:532–551. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
