

A Multifaceted Approach to Interpreting Reaction Time Deficits After Adolescent Concussion
- PMID: 36701688
- PMCID: PMC10895397
- DOI: 10.4085/1062-6050-0566.22
A Multifaceted Approach to Interpreting Reaction Time Deficits After Adolescent Concussion
Abstract
Context: Reaction time (RT) is a critical element of return to participation (RTP), and impairments have been linked to subsequent injury after a concussion. Current RT assessments have limitations in clinical feasibility and in the identification of subtle deficits after concussion symptom resolution.
Objectives: To examine the utility of RT measurements (clinical drop stick, simple stimulus-response, single-task Stroop, and dual-task Stroop) to differentiate between adolescents with concussion and uninjured control individuals at initial assessment and RTP.
Design: Prospective cohort study.
Setting: A pediatric sports medicine center associated with a regional tertiary care hospital.
Patients or other participants: Twenty-seven adolescents with a concussion (mean age = 14.8 ± 2.1 years; 52% female; tested 7.0 ± 3.3 days postconcussion) and 21 uninjured control individuals (mean age = 15.5 ± 1.6 years; 48% female).
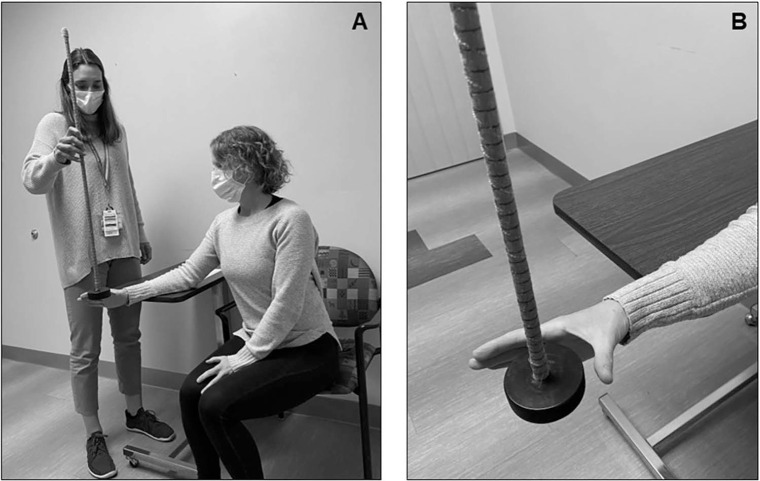
Main outcome measure(s): Participants completed the Post-Concussion Symptoms Inventory (PCSI) and a battery of RT tests: clinical drop stick, simple stimulus-response, single-task Stroop, and dual-task Stroop.
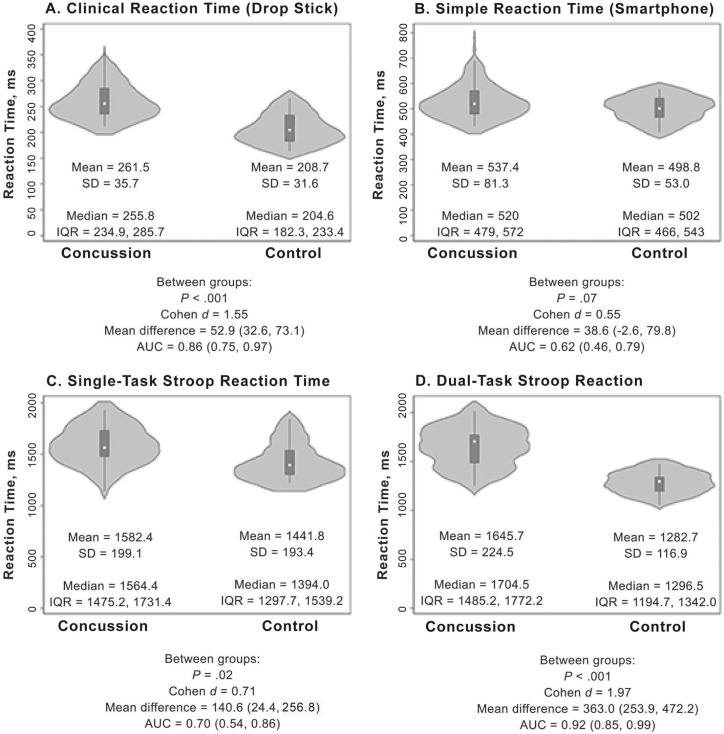
Results: The concussion group demonstrated slower clinical drop stick (β = 58.8; 95% CI = 29.2, 88.3; P < .001) and dual-task Stroop (β = 464.2; 95% CI = 318.4, 610.0; P < .001) RT measures at the initial assessment than the uninjured control group. At 1-month follow up, the concussion group displayed slower clinical drop stick (238.9 ± 25.9 versus 188.1 ± 21.7 milliseconds; P < .001; d = 2.10), single-task Stroop (1527.8 ± 204.5 versus 1319.8 ± 133.5 milliseconds; P = .001; d = 1.20), and dual-task Stroop (1549.9 ± 264.7 versus 1341.5 ± 114.7 milliseconds; P = .002; d = 1.04) RT than the control group, respectively, while symptom severity was similar between groups (7.4 ± 11.2 versus 5.3 ± 6.5; P = .44; d = 0.24). Classification accuracy and area under the curve (AUC) values were highest for the clinical drop stick (85.1% accuracy, AUC = 0.86, P < .001) and dual-task Stroop (87.2% accuracy, AUC = 0.92, P < .002) RT variables at initial evaluation.
Conclusions: Adolescents recovering from concussion may have initial RT deficits that persist despite symptom recovery. The clinical drop stick and dual-task Stroop RT measures demonstrated high clinical utility given high classification accuracy, sensitivity, and specificity to detect postconcussion RT deficits and may be considered for initial and RTP assessment.
Keywords: adolescent athletes; mild traumatic brain injuries; return to participation; sports.
© by the National Athletic Trainers’ Association, Inc.
Figures
Similar articles
-
Gait and Quiet-Stance Performance Among Adolescents After Concussion-Symptom Resolution.J Athl Train. 2017 Dec;52(12):1089-1095. doi: 10.4085/1062-6050-52.11.23. Epub 2017 Nov 20. J Athl Train. 2017. PMID: 29154694 Free PMC article.
-
Clinical versus Functional Reaction Time: Implications for Postconcussion Management.Med Sci Sports Exerc. 2020 Aug;52(8):1650-1657. doi: 10.1249/MSS.0000000000002300. Med Sci Sports Exerc. 2020. PMID: 32053547 Clinical Trial.
-
The Association between Dual-Task Gait after Concussion and Prolonged Symptom Duration.J Neurotrauma. 2017 Dec 1;34(23):3288-3294. doi: 10.1089/neu.2017.5191. Epub 2017 Oct 16. J Neurotrauma. 2017. PMID: 28895490
-
American Medical Society for Sports Medicine position statement: concussion in sport.Br J Sports Med. 2013 Jan;47(1):15-26. doi: 10.1136/bjsports-2012-091941. Br J Sports Med. 2013. PMID: 23243113 Review.
-
Concussed athletes walk slower than non-concussed athletes during cognitive-motor dual-task assessments but not during single-task assessments 2 months after sports concussion: a systematic review and meta-analysis using individual participant data.Br J Sports Med. 2020 Jan;54(2):94-101. doi: 10.1136/bjsports-2018-100164. Epub 2019 Jul 22. Br J Sports Med. 2020. PMID: 31331944
Cited by
-
Validity and Reliability of Methods to Assess Movement Deficiencies Following Concussion: A COSMIN Systematic Review.Sports Med Open. 2023 Aug 14;9(1):76. doi: 10.1186/s40798-023-00625-0. Sports Med Open. 2023. PMID: 37578611 Free PMC article.
-
The Significance of Off-Season Tailor-Made Baseline Measurements in the Assessment of Post-Concussion in University Athletes.Brain Sci. 2024 Jul 12;14(7):698. doi: 10.3390/brainsci14070698. Brain Sci. 2024. PMID: 39061438 Free PMC article.
-
Clinical Measures Associated with Subsequent Injury after Adolescent Concussion: A Prospective Cohort Study.Med Sci Sports Exerc. 2025 Feb 1;57(2):252-259. doi: 10.1249/MSS.0000000000003575. Med Sci Sports Exerc. 2025. PMID: 39733225
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
