

Novel severe oculocutaneous manifestations of human monkeypox virus infection and their historical analogues
- PMID: 36702137
- PMCID: PMC9870321
- DOI: 10.1016/S1473-3099(22)00869-6
Novel severe oculocutaneous manifestations of human monkeypox virus infection and their historical analogues
Abstract
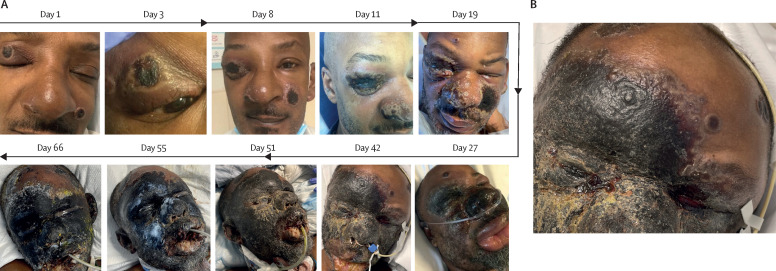
WHO has declared human mpox (formerly known as monkeypox) a global public health emergency since July, 2022. When case numbers were increasing, so did clinicians' exposures to new elements of the disease. Additionally, the burden of mpox is particularly apparent in immunocompromised patients, who can have more variable and severe manifestations of disease across organ systems. In this Grand Round, we report novel and severe oculocutaneous manifestations of mpox in this population, which are both sight and life threatening. Specifically, we highlight two patients with mpox and AIDS who had refractory skin necrosis that progressed to either ocular compromise or panfacial gangrene, or both. Both patients ultimately died due to systemic complications of their infections. Through clinical analogies, we show how past experiences with related orthopoxviruses, such as variola virus (smallpox) and vaccinia virus, can add useful context for understanding and treating these new disease states. We suspect that in patients who are immunocompromised, monkeypox virus can clinically evolve not only via viraemia but also through direct intradermal spread. We propose that intradermal spread occurs by a process clinically and immunologically analogous to progressive vaccinia, a complication previously seen after conventional smallpox vaccination. We share evidence in support of this theory and implications regarding early management and post-exposure prophylaxis for at-risk populations. Content note: this Grand Round contains graphic images of mpox lesions of the eyes and face.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures



Similar articles
-
Human monkeypox virus in the shadow of the COVID-19 pandemic.J Infect Public Health. 2023 Aug;16(8):1149-1157. doi: 10.1016/j.jiph.2023.05.013. Epub 2023 May 13. J Infect Public Health. 2023. PMID: 37269693 Free PMC article. Review.
-
Interim Clinical Treatment Considerations for Severe Manifestations of Mpox - United States, February 2023.MMWR Morb Mortal Wkly Rep. 2023 Mar 3;72(9):232-243. doi: 10.15585/mmwr.mm7209a4. MMWR Morb Mortal Wkly Rep. 2023. PMID: 36862595 Free PMC article.
-
Monkeypox (Mpox) outbreak during COVID-19 pandemic-Past and the future.J Med Virol. 2023 Apr;95(4):e28701. doi: 10.1002/jmv.28701. J Med Virol. 2023. PMID: 36951352 Review.
-
Therapeutic strategies for human poxvirus infections: Monkeypox (mpox), smallpox, molluscipox, and orf.Travel Med Infect Dis. 2023 Mar-Apr;52:102528. doi: 10.1016/j.tmaid.2022.102528. Epub 2022 Dec 17. Travel Med Infect Dis. 2023. PMID: 36539022 Free PMC article. Review.
-
Mpox: Rapid Evidence Review.Am Fam Physician. 2023 Jul;108(1):78-83. Am Fam Physician. 2023. PMID: 37440743 Review.
Cited by
-
Spectrum of ophthalmic manifestations in monkeypox virus infection worldwide: Systematic review and meta-analysis.Heliyon. 2023 Jul 22;9(8):e18561. doi: 10.1016/j.heliyon.2023.e18561. eCollection 2023 Aug. Heliyon. 2023. PMID: 37576249 Free PMC article. Review.
-
A Case of Sustained Viral Shedding of Mpox With Ocular Involvement Resulting in Vision Loss.Open Forum Infect Dis. 2023 Dec 14;11(1):ofad632. doi: 10.1093/ofid/ofad632. eCollection 2024 Jan. Open Forum Infect Dis. 2023. PMID: 38264094 Free PMC article.
-
Ocular manifestations of mpox.Curr Opin Ophthalmol. 2024 Sep 1;35(5):423-429. doi: 10.1097/ICU.0000000000001066. Epub 2024 Jun 6. Curr Opin Ophthalmol. 2024. PMID: 38847744 Free PMC article. Review.
-
Fatal Case of Progressive Mpox in a Patient with AIDS-Viral Enteropathy and Malabsorption Demanding the Use of Full Parenteral ARV and Endovenous Cidofovir.Infect Dis Rep. 2023 Mar 16;15(2):171-179. doi: 10.3390/idr15020018. Infect Dis Rep. 2023. PMID: 36960970 Free PMC article.
-
Mpox and Lessons Learned in the Light of the Recent Outbreak: A Narrative Review.Viruses. 2024 Oct 16;16(10):1620. doi: 10.3390/v16101620. Viruses. 2024. PMID: 39459952 Free PMC article. Review.
References
-
- Centers for Disease Control and Prevention 2022 outbreak cases and data. 2022. https://www.cdc.gov/poxvirus/monkeypox/response/2022/index.html
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
