

Connectomic Basis for Tremor Control in Stereotactic Radiosurgical Thalamotomy
- PMID: 36702499
- PMCID: PMC9891328
- DOI: 10.3174/ajnr.A7778
Connectomic Basis for Tremor Control in Stereotactic Radiosurgical Thalamotomy
Abstract
Background and purpose: Given the increased use of stereotactic radiosurgical thalamotomy and other ablative therapies for tremor, new biomarkers are needed to improve outcomes. Using resting-state fMRI and MR tractography, we hypothesized that a "connectome fingerprint" can predict tremor outcomes and potentially serve as a targeting biomarker for stereotactic radiosurgical thalamotomy.
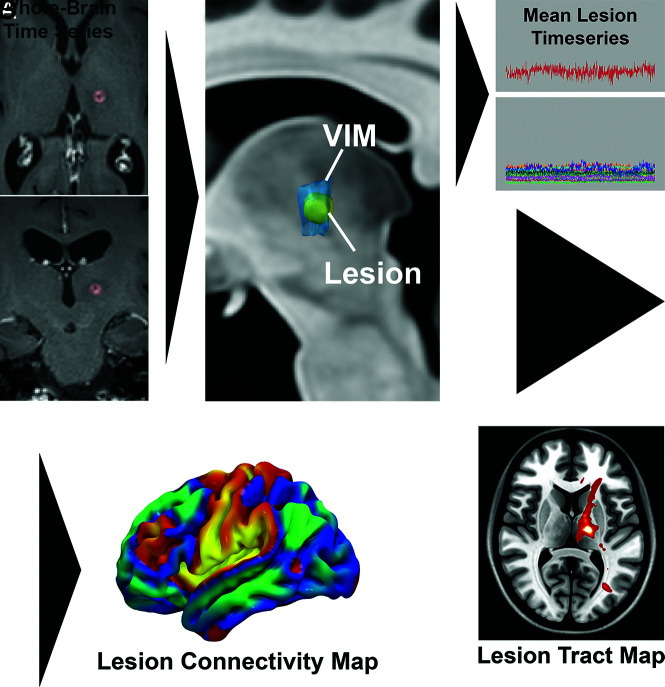
Materials and methods: We evaluated 27 patients who underwent unilateral stereotactic radiosurgical thalamotomy for essential tremor or tremor-predominant Parkinson disease. Percentage postoperative improvement in the contralateral limb Fahn-Tolosa-Marin Clinical Tremor Rating Scale (TRS) was the primary end point. Connectome-style resting-state fMRI and MR tractography were performed before stereotactic radiosurgery. Using the final lesion volume as a seed, "connectivity fingerprints" representing ideal connectivity maps were generated as whole-brain R-maps using a voxelwise nonparametric Spearman correlation. A leave-one-out cross-validation was performed using the generated R-maps.
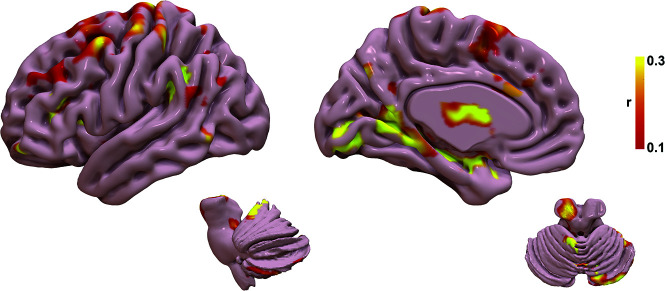
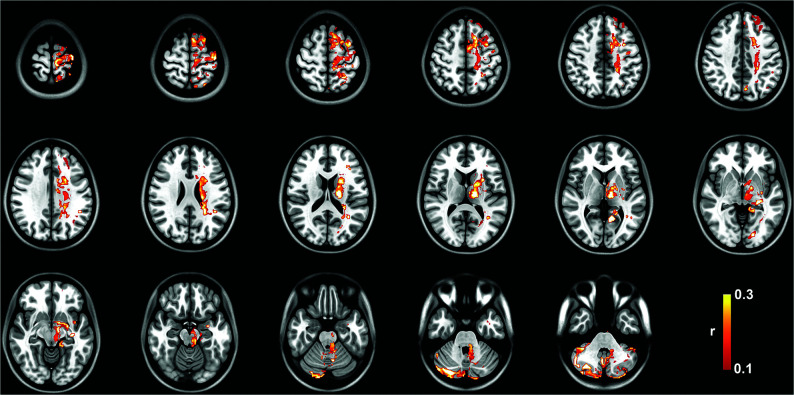
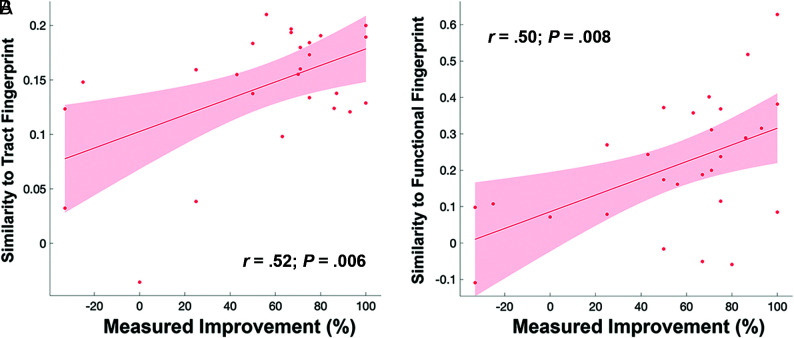
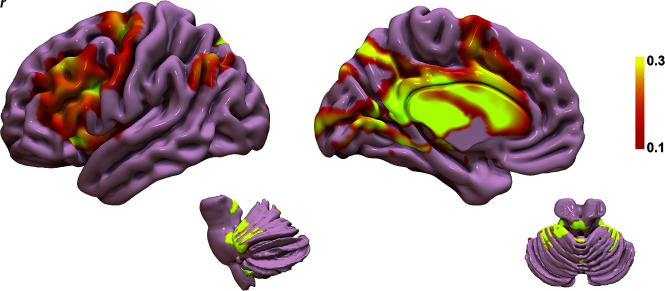
Results: The mean improvement in the contralateral tremor score was 55.1% (SD, 38.9%) at a mean follow-up of 10.0 (SD, 5.0) months. Structural connectivity correlated with contralateral TRS improvement (r = 0.52; P = .006) and explained 27.0% of the variance in outcome. Functional connectivity correlated with contralateral TRS improvement (r = 0.50; P = .008) and explained 25.0% of the variance in outcome. Nodes most correlated with tremor improvement corresponded to areas of known network dysfunction in tremor, including the cerebello-thalamo-cortical pathway and the primary and extrastriate visual cortices.
Conclusions: Stereotactic radiosurgical targets with a distinct connectivity profile predict improvement in tremor after treatment. Such connectomic fingerprints show promise for developing patient-specific biomarkers to guide therapy with stereotactic radiosurgical thalamotomy.
Trial registration: ClinicalTrials.gov NCT03305588.
© 2023 by American Journal of Neuroradiology.
Figures
Similar articles
-
Connectomic-guided stereotactic radiosurgery thalamotomy for tremor: a patient-specific approach to enhance outcomes.J Neurosurg. 2025 Feb 14;143(1):53-62. doi: 10.3171/2024.10.JNS24753. Print 2025 Jul 1. J Neurosurg. 2025. PMID: 39951712
-
Pretherapeutic resting-state fMRI profiles are associated with MR signature volumes after stereotactic radiosurgical thalamotomy for essential tremor.J Neurosurg. 2018 Dec 1;129(Suppl1):63-71. doi: 10.3171/2018.7.GKS18752. J Neurosurg. 2018. PMID: 30544321
-
Ventrolateral Motor Thalamus Abnormal Connectivity in Essential Tremor Before and After Thalamotomy: A Resting-State Functional Magnetic Resonance Imaging Study.World Neurosurg. 2018 May;113:e453-e464. doi: 10.1016/j.wneu.2018.02.055. Epub 2018 Feb 21. World Neurosurg. 2018. PMID: 29475059
-
Stereotactic robot-assisted MRI-guided laser interstitial thermal therapy thalamotomy for medically intractable Holmes tremor: a pilot study and literature review.Neurosurg Focus. 2024 Nov 1;57(5):E9. doi: 10.3171/2024.8.FOCUS24444. Neurosurg Focus. 2024. PMID: 39486081 Review.
-
Focused ultrasound and other lesioning in the treatment of tremor.J Neurol Sci. 2022 Apr 15;435:120193. doi: 10.1016/j.jns.2022.120193. Epub 2022 Feb 19. J Neurol Sci. 2022. PMID: 35259650 Review.
Cited by
-
The variation of functional connectivity and activity before and after thalamotomy surgery (review).Front Hum Neurosci. 2023 Apr 28;17:1108888. doi: 10.3389/fnhum.2023.1108888. eCollection 2023. Front Hum Neurosci. 2023. PMID: 37187943 Free PMC article. Review.
-
The rubral wing and its connectome.Neuroimage Clin. 2025 Jul 20;48:103849. doi: 10.1016/j.nicl.2025.103849. Online ahead of print. Neuroimage Clin. 2025. PMID: 40701135 Free PMC article.
-
Stereotactic radiosurgery in the treatment of essential tremor - a systematic review.Front Neurol. 2024 Apr 3;15:1370091. doi: 10.3389/fneur.2024.1370091. eCollection 2024. Front Neurol. 2024. PMID: 38633530 Free PMC article.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical