

Histologic Features of Syphilitic Gastritis: A Rare but Resurging Imitator of Common Diseases
- PMID: 36702577
- PMCID: PMC10452963
- DOI: 10.1093/ajcp/aqac153
Histologic Features of Syphilitic Gastritis: A Rare but Resurging Imitator of Common Diseases
Erratum in
-
Correction to: Histologic Features of Syphilitic Gastritis: A Rare but Resurging Imitator of Common Diseases.Am J Clin Pathol. 2023 Mar 13;159(3):305. doi: 10.1093/ajcp/aqad028. Am J Clin Pathol. 2023. PMID: 36852866 Free PMC article. No abstract available.
Abstract
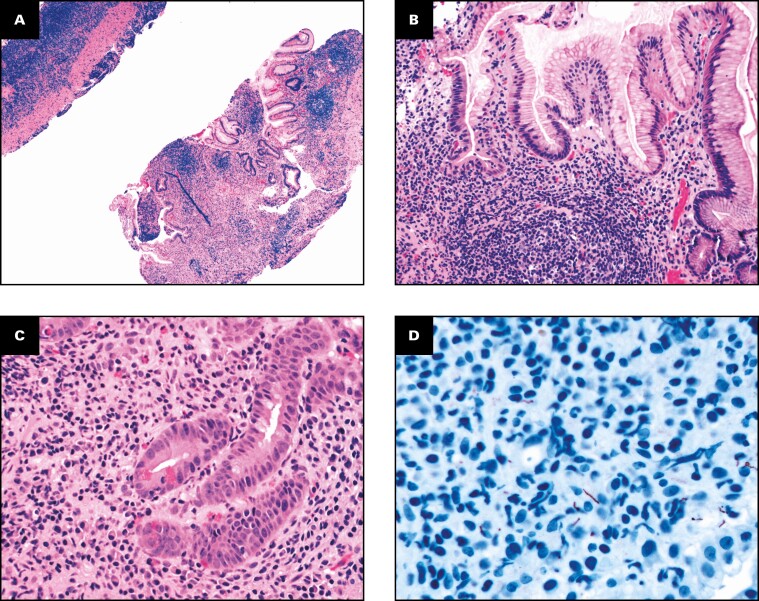
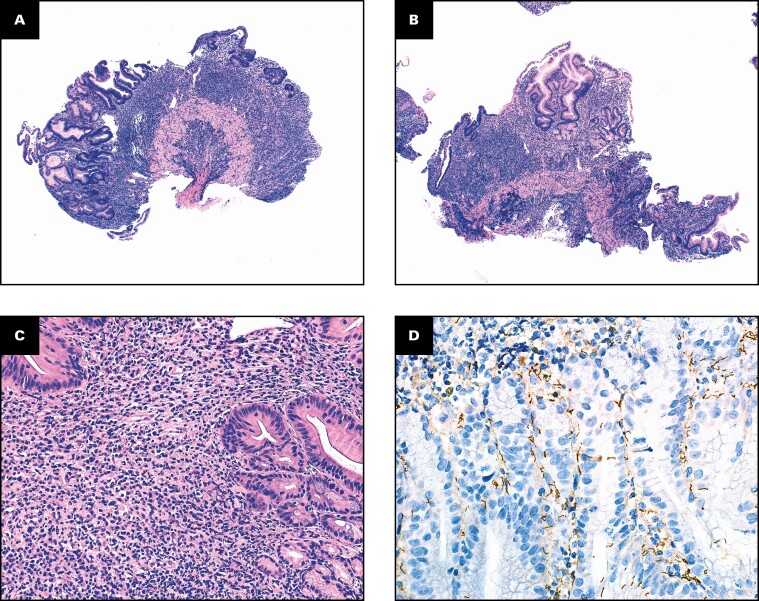
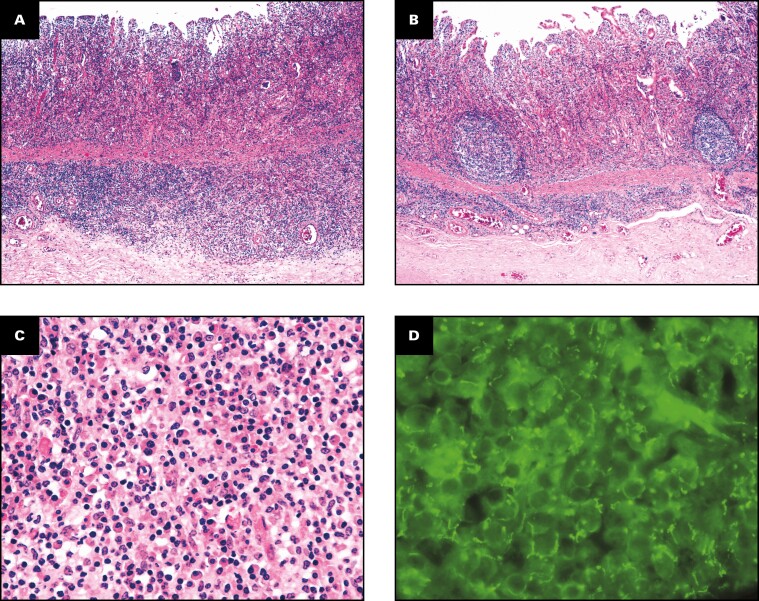
Objectives: The range of histopathologic features of gastric syphilis is not well described. Here we describe the clinicopathologic findings of eight patients with syphilitic gastritis.
Methods: A search of our Pathology Data System (2003-2022) and multiple other institutions identified eight patients with syphilitic gastritis. Clinical information, pathology reports, and available slides were reviewed.
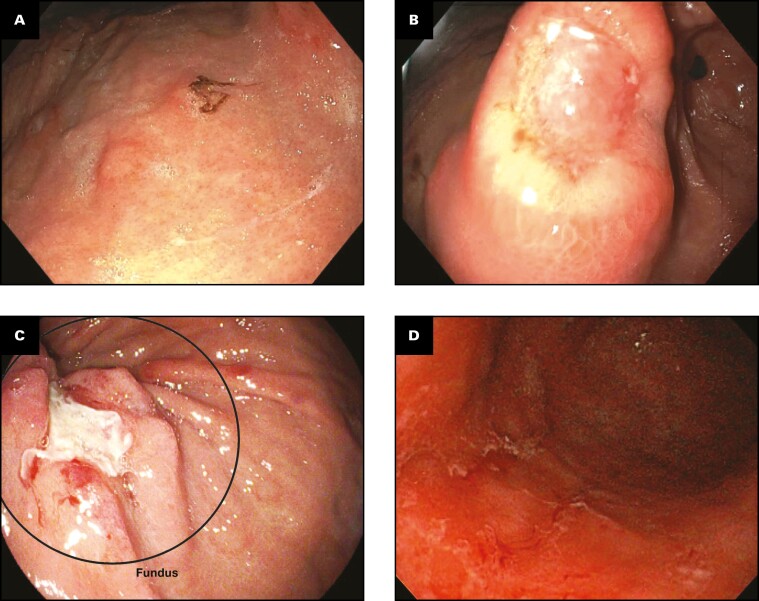
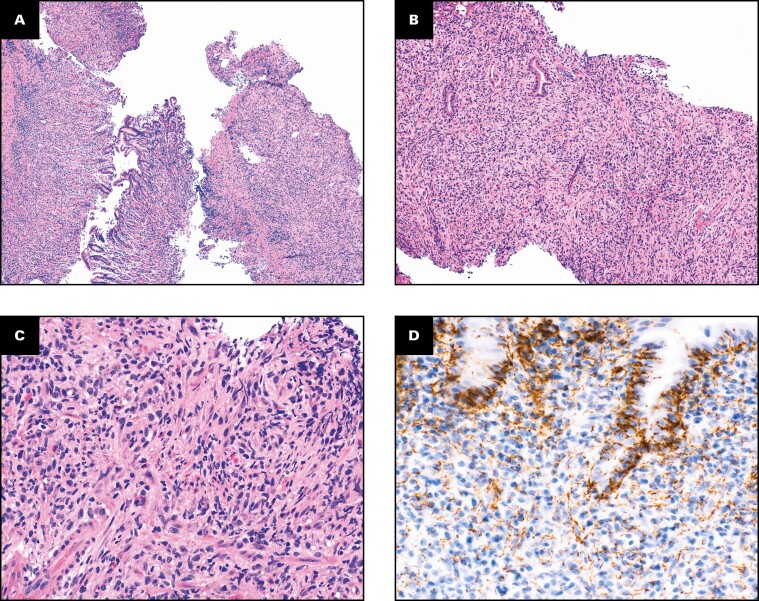
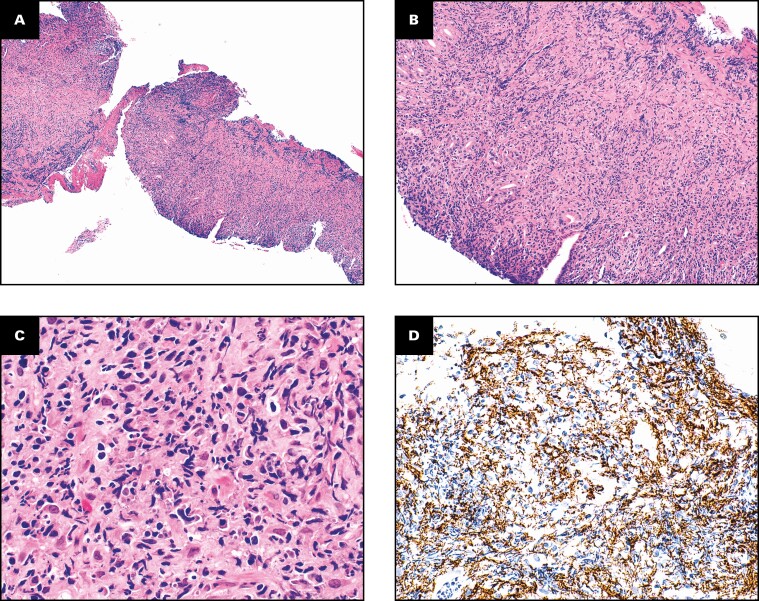
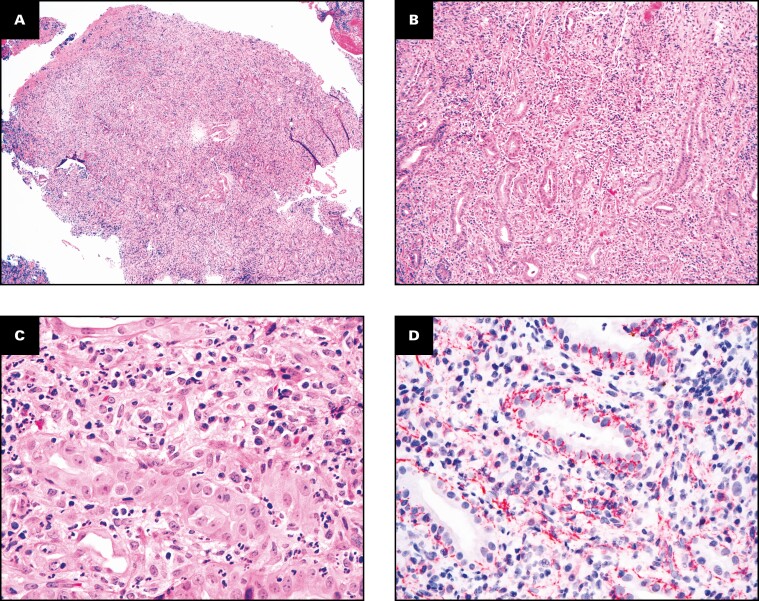
Results: Lesions predominated in middle-aged adults (mean age, 47.2 years; range, 23-61 years) with a propensity for men (n = 7). Three patients had a documented history of human immunodeficiency virus. Clinical presentations included weight loss, abdominal pain, hematochezia, fever, dyspepsia, nausea and vomiting, hematemesis, anemia, and early satiety. Endoscopic findings included ulcerations, erosions, abnormal mucosa, and nodularity. All specimens shared an active chronic gastritis pattern with intense lymphohistiocytic infiltrates, variable plasma cells, and gland loss. Prominent lymphoid aggregates were seen in four specimens. The diagnosis was confirmed either by immunostain for Treponema pallidum (n = 7) or by direct immunofluorescence staining and real-time polymerase chain reaction (n = 1). All patients with available follow-up data showed resolution of symptoms after antibiotic therapy (n = 4).
Conclusions: Recognition of the histologic pattern of syphilitic gastritis facilitates timely treatment, prevents further transmission, and avoids unnecessarily aggressive treatment.
Keywords: Treponema pallidum; Gastric pathology; Gastritis; Human immunodeficiency virus (HIV); Lymphoma; Men who have sex with men (MSM); Syphilis.
© The Author(s) 2023. Published by Oxford University Press on behalf of American Society for Clinical Pathology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Syphilitic and lymphogranuloma venereum (LGV) proctocolitis: clues to a frequently missed diagnosis.Am J Surg Pathol. 2013 Jan;37(1):38-46. doi: 10.1097/PAS.0b013e31826a523e. Am J Surg Pathol. 2013. PMID: 23095509
-
Case of secondary syphilis presenting with unusual complications: syphilitic proctitis, gastritis, and hepatitis.J Clin Microbiol. 2011 Dec;49(12):4394-6. doi: 10.1128/JCM.01240-11. Epub 2011 Oct 12. J Clin Microbiol. 2011. PMID: 21998411 Free PMC article.
-
Treponema pallidum immunostain distinguishing syphilitic gastritis from Helicobacter pylori-associated gastritis.Hum Pathol. 2010 Apr;41(4):617-9; author reply 619. doi: 10.1016/j.humpath.2010.01.003. Hum Pathol. 2010. PMID: 20226965 No abstract available.
-
Novelty in the gut: a review of the gastrointestinal manifestations of syphilis.Scand J Gastroenterol. 2024 Dec;59(12):1306-1313. doi: 10.1080/00365521.2024.2429676. Epub 2024 Nov 14. Scand J Gastroenterol. 2024. PMID: 39540599 Review.
-
The clinical relevance of endoscopic and histologic inflammation of gastroduodenal mucosa in dyspepsia of unknown origin.Scand J Gastroenterol. 1989 May;24(4):385-95. doi: 10.3109/00365528909093064. Scand J Gastroenterol. 1989. PMID: 2675301 Review.
Cited by
-
An unusual cause of epigastric pain: Gastric syphilis.J Gen Fam Med. 2024 Jun 24;25(5):282-283. doi: 10.1002/jgf2.712. eCollection 2024 Sep. J Gen Fam Med. 2024. PMID: 39574550 Free PMC article.
References
-
- Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2019. Atlanta, GA: US Department of Health and Human Services; 2021.
-
- Atten MJ, Attar BM, Teopengco E, et al. . Gastric syphilis: a disease with multiple manifestations. Am J Gastroenterol. 1994;89:2227-2229. - PubMed
-
- Mylona EE, Baraboutis IG, Papastamopoulos V, et al. . Gastric syphilis: a systematic review of published cases of the last 50 years. Sex Transm Dis. 2010;37:177-183. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
