

The potential of point-of-care diagnostics to optimise prehospital trauma triage: a systematic review of literature
- PMID: 36703080
- PMCID: PMC10449679
- DOI: 10.1007/s00068-023-02226-8
The potential of point-of-care diagnostics to optimise prehospital trauma triage: a systematic review of literature
Abstract
Purpose: In the prehospital care of potentially seriously injured patients resource allocation adapted to injury severity (triage) is a challenging. Insufficiently specified triage algorithms lead to the unnecessary activation of a trauma team (over-triage), resulting in ineffective consumption of economic and human resources. A prehospital trauma triage algorithm must reliably identify a patient bleeding or suffering from significant brain injuries. By supplementing the prehospital triage algorithm with in-hospital established point-of-care (POC) tools the sensitivity of the prehospital triage is potentially increased. Possible POC tools are lactate measurement and sonography of the thorax, the abdomen and the vena cava, the sonographic intracranial pressure measurement and the capnometry in the spontaneously breathing patient. The aim of this review was to assess the potential and to determine diagnostic cut-off values of selected instrument-based POC tools and the integration of these findings into a modified ABCDE based triage algorithm.
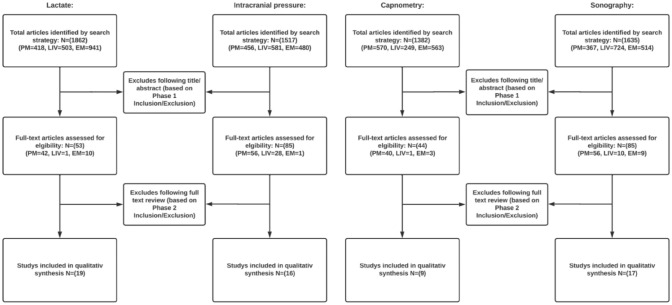
Methods: A systemic search on MEDLINE via PubMed, LIVIVO and Embase was performed for patients in an acute setting on the topic of preclinical use of the selected POC tools to identify critical cranial and peripheral bleeding and the recognition of cerebral trauma sequelae. For the determination of the final cut-off values the selected papers were assessed with the Newcastle-Ottawa scale for determining the risk of bias and according to various quality criteria to subsequently be classified as suitable or unsuitable. PROSPERO Registration: CRD 42022339193.
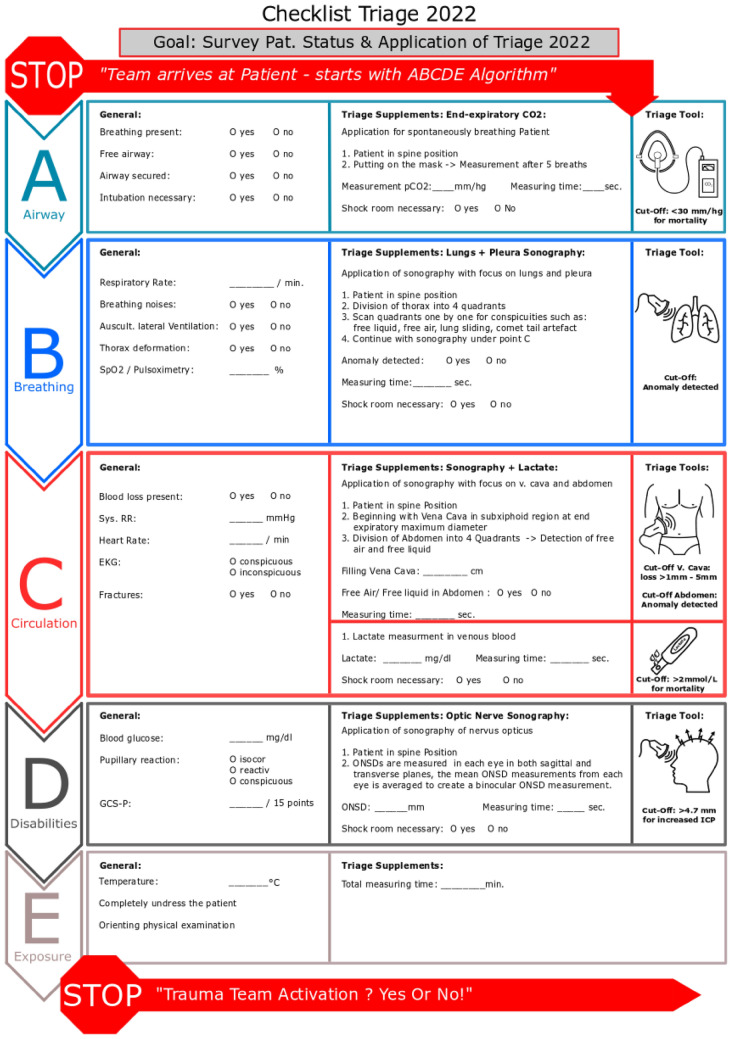
Results: 267 papers were identified as potentially relevant and processed in full text form. 61 papers were selected for the final evaluation, of which 13 papers were decisive for determining the cut-off values. Findings illustrate that a preclinical use of point-of-care diagnostic is possible. These adjuncts can provide additional information about the expected long-term clinical course of patients. Clinical outcomes like mortality, need of emergency surgery, intensive care unit stay etc. were taken into account and a hypothetic cut-off value for trauma team activation could be determined for each adjunct. The cut-off values are as follows: end-expiratory CO2: < 30 mm/hg; sonography thorax + abdomen: abnormality detected; lactate measurement: > 2 mmol/L; optic nerve diameter in sonography: > 4.7 mm.
Discussion: A preliminary version of a modified triage algorithm with hypothetic cut-off values for a trauma team activation was created. However, further studies should be conducted to optimize the final cut-off values in the future. Furthermore, studies need to evaluate the practical application of the modified algorithm in terms of feasibility (e.g. duration of application, technique, etc.) and the effects of the new algorithm on over-triage. Limiting factors are the restriction with the search and the heterogeneity between the studies (e.g. varying measurement devices, techniques etc.).
Keywords: Advanced trauma life support care; Emergency medical service; Focused assessment with sonography for trauma; Point-of-care testing; Triage.
© 2023. The Author(s).
Conflict of interest statement
The authors have no competing interests to declare that are relevant to the content of this article.
References
-
- Deutsche Gesellschaft für Unfallchirurgie e.V. (DGU). Jahresbericht 2021—TraumaRegister DGU®für das Unfalljahr. 2020. https://www.traumaregister-dgu.de/fileadmin/user_upload/TR-DGU_Jahresber....
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
