

Age-adjusted Charlson Comorbidity Index as effective predictor for in-hospital mortality of patients with cardiac arrest: a retrospective study
- PMID: 36703122
- PMCID: PMC9878885
- DOI: 10.1186/s12873-022-00769-4
Age-adjusted Charlson Comorbidity Index as effective predictor for in-hospital mortality of patients with cardiac arrest: a retrospective study
Abstract
Background: Cardiac arrest is currently one of the leading causes of mortality in clinical practice, and the Charlson Comorbidity Index (CCI) is widely utilized to assess the severity of comorbidities. We aimed to evaluate the relationship between the age-adjusted CCI score and in-hospital mortality in intensive care unit (ICU) patients with the diagnosis of cardiac arrest, which is important but less explored previously.
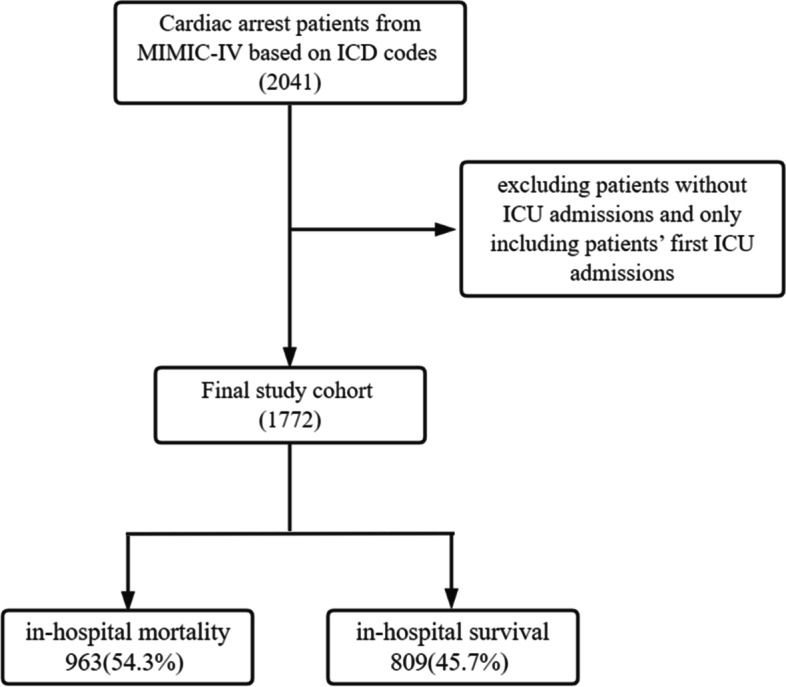
Methods: This was a retrospective study including patients aged over 18 years from the MIMIC-IV database. We calculated the age-adjusted CCI using age information and ICD codes. The univariate analysis for varied predictors' differences between the survival and the non-survival groups was performed. In addition, a multiple factor analysis was conducted based on logistic regression analysis with the primary result set as hospitalization death. An additional multivariate regression analysis was conducted to estimate the influence of hospital and ICU stay.
Results: A total of 1772 patients were included in our study, with median age of 66, among which 705 (39.8%) were female. Amongst these patients, 963 (54.3%) died during the hospitalization period. Patients with higher age-adjusted CCI scores had a higher likelihood of dying during hospitalization (P < 0.001; OR: 1.109; 95% CI: 1.068-1.151). With the age-adjusted CCI incorporated into the predictive model, the area under the receiver operating characteristic curve was 0.794 (CI: 0.773-0.814), showing that the prediction model is effective. Additionally, patients with higher age-adjusted CCI scores stayed longer in the hospital (P = 0.026, 95% CI: 0.056-0.896), but there was no significant difference between patients with varied age-adjusted CCI scores on the days of ICU stay.
Conclusion: The age-adjusted CCI is a valid indicator to predict death in ICU patients with cardiac arrest, which can offer enlightenment for both theory literatures and clinical practice.
Keywords: Age-adjusted Charlson Comorbidity Index; Cardiac arrest; In-hospital mortality; Length of hospital stay.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Correlation between Charlson comorbidity index and surgical prognosis in elderly patients with femoral neck fractures: a retrospective study.BMC Musculoskelet Disord. 2024 Aug 29;25(1):678. doi: 10.1186/s12891-024-07814-2. BMC Musculoskelet Disord. 2024. PMID: 39210355 Free PMC article.
-
Impact of Charlson Comorbidity Index on in-hospital mortality of patients with hyperglycemic crises: A propensity score matching analysis.J Eval Clin Pract. 2024 Sep;30(6):977-988. doi: 10.1111/jep.14005. Epub 2024 May 7. J Eval Clin Pract. 2024. PMID: 38713640
-
The risk-adjusted Charlson comorbidity index as a new predictor of one-year mortality rate in elderly Chinese patients who underwent hip fracture surgery.Orthop Traumatol Surg Res. 2021 May;107(3):102860. doi: 10.1016/j.otsr.2021.102860. Epub 2021 Feb 17. Orthop Traumatol Surg Res. 2021. PMID: 33609760
-
Charlson Comorbidity Index: A Critical Review of Clinimetric Properties.Psychother Psychosom. 2022;91(1):8-35. doi: 10.1159/000521288. Epub 2022 Jan 6. Psychother Psychosom. 2022. PMID: 34991091 Review.
-
Charlson comorbidity index and a composite of poor outcomes in COVID-19 patients: A systematic review and meta-analysis.Diabetes Metab Syndr. 2020 Nov-Dec;14(6):2103-2109. doi: 10.1016/j.dsx.2020.10.022. Epub 2020 Oct 28. Diabetes Metab Syndr. 2020. PMID: 33161221 Free PMC article.
Cited by
-
Comparing the outcomes and costs of cardiac monitoring with implantable loop recorders and mobile cardiac outpatient telemetry following stroke using real-world evidence.J Comp Eff Res. 2024 Jun;13(6):e240008. doi: 10.57264/cer-2024-0008. Epub 2024 Apr 11. J Comp Eff Res. 2024. PMID: 38602503 Free PMC article.
-
Factors affecting do-not-attempt-resuscitation (DNAR) decisions among adult patients in the emergency department of a general tertiary teaching hospital in China: a retrospective observational study.BMJ Open. 2023 Oct 10;13(10):e075714. doi: 10.1136/bmjopen-2023-075714. BMJ Open. 2023. PMID: 37816558 Free PMC article.
-
Effectiveness and Safety of Endoscopic Submucosal Dissection for Colorectal Neoplasm in Patients with High Charlson Comorbidity Index Score: A HASID Multicenter Study.J Clin Med. 2023 Sep 28;12(19):6255. doi: 10.3390/jcm12196255. J Clin Med. 2023. PMID: 37834899 Free PMC article.
-
Age‑adjusted Charlson comorbidity index and in‑hospital mortality in critically ill patients with cardiogenic shock: A retrospective cohort study.Exp Ther Med. 2023 May 5;25(6):299. doi: 10.3892/etm.2023.11998. eCollection 2023 Jun. Exp Ther Med. 2023. PMID: 37229315 Free PMC article.
-
Construction and validation of prognostic model for ICU mortality in cardiac arrest patients: an interpretable machine learning modeling approach.Eur J Med Res. 2025 Apr 24;30(1):328. doi: 10.1186/s40001-025-02588-2. Eur J Med Res. 2025. PMID: 40275415 Free PMC article.
References
-
- Yan S, Gan Y, Jiang N, Wang R, Chen Y, Luo Z, Zong Q, Chen S, Lv C. The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: a systematic review and meta-analysis. Crit Care. 2020;24(1):61. doi: 10.1186/s13054-020-2773-2. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
