

Prioritization of intervention domains to prevent cardiovascular disease: a country-level case study using global burden of disease and local data
- PMID: 36703150
- PMCID: PMC9878487
- DOI: 10.1186/s12963-023-00301-1
Prioritization of intervention domains to prevent cardiovascular disease: a country-level case study using global burden of disease and local data
Abstract
Aim: We aimed to combine Global Burden of Disease (GBD) Study data and local data to identify the highest priority intervention domains for preventing cardiovascular disease (CVD) in the case study country of Aotearoa New Zealand (NZ).
Methods: Risk factor data for CVD in NZ were extracted from the GBD using the "GBD Results Tool." We prioritized risk factor domains based on consideration of the size of the health burden (disability-adjusted life years [DALYs]) and then by the domain-specific interventions that delivered the highest health gains and cost-savings.
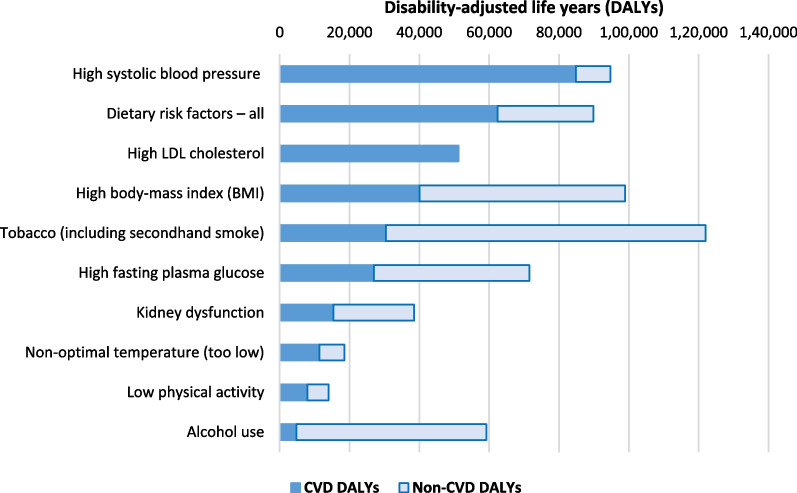
Results: Based on the size of the CVD health burden in DALYs, the five top prioritized risk factor domains were: high systolic blood pressure (84,800 DALYs; 5400 deaths in 2019), then dietary risk factors, then high LDL cholesterol, then high BMI and then tobacco (30,400 DALYs; 1400 deaths). But if policy-makers aimed to maximize health gain and cost-savings from specific interventions that have been studied, then they would favor the dietary risk domain (e.g., a combined fruit and vegetable subsidy plus a sugar tax produced estimated lifetime savings of 894,000 health-adjusted life years and health system cost-savings of US$11.0 billion; both 3% discount rate). Other potential considerations for prioritization included the potential for total health gain that includes non-CVD health loss and potential for achieving relatively greater per capita health gain for Māori (Indigenous) to reduce health inequities.
Conclusions: We were able to show how CVD risk factor domains could be systematically prioritized using a mix of GBD and country-level data. Addressing high systolic blood pressure would be the top ranked domain if policy-makers focused just on the size of the health loss. But if policy-makers wished to maximize health gain and cost-savings using evaluated interventions, dietary interventions would be prioritized, e.g., food taxes and subsidies.
Keywords: Burden of disease; Cardiovascular disease; DALYs; Health economic evaluation; Preventive interventions; Prioritization; Risk factors.
© 2023. The Author(s).
Conflict of interest statement
Not applicable.
Figures
Similar articles
-
Global burden of cardiovascular disease attributable to metabolic risk factors, 1990-2019: an analysis of observational data from a 2019 Global Burden of Disease study.BMJ Open. 2023 May 12;13(5):e069397. doi: 10.1136/bmjopen-2022-069397. BMJ Open. 2023. PMID: 37173115 Free PMC article.
-
Cardiovascular disease burden attributable to dietary risk factors from 1990 to 2019: A systematic analysis of the Global Burden of Disease study.Nutr Metab Cardiovasc Dis. 2022 Apr;32(4):897-907. doi: 10.1016/j.numecd.2021.11.012. Epub 2021 Nov 29. Nutr Metab Cardiovasc Dis. 2022. PMID: 35067445
-
The health gains and cost savings of dietary salt reduction interventions, with equity and age distributional aspects.BMC Public Health. 2016 May 23;16:423. doi: 10.1186/s12889-016-3102-1. BMC Public Health. 2016. PMID: 27216490 Free PMC article.
-
Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019.Lancet Psychiatry. 2022 Feb;9(2):137-150. doi: 10.1016/S2215-0366(21)00395-3. Epub 2022 Jan 10. Lancet Psychiatry. 2022. PMID: 35026139 Free PMC article.
-
Burden of Neurological Disorders Across the US From 1990-2017: A Global Burden of Disease Study.JAMA Neurol. 2021 Feb 1;78(2):165-176. doi: 10.1001/jamaneurol.2020.4152. JAMA Neurol. 2021. PMID: 33136137 Free PMC article.
Cited by
-
Global and national burden of atherosclerosis from 1990 to 2019: trend analysis based on the Global Burden of Disease Study 2019.Chin Med J (Engl). 2023 Oct 20;136(20):2442-2450. doi: 10.1097/CM9.0000000000002839. Epub 2023 Sep 5. Chin Med J (Engl). 2023. PMID: 37677929 Free PMC article.
-
Global, regional, and national burden of cardiovascular diseases in youths and young adults aged 15-39 years in 204 countries/territories, 1990-2019: a systematic analysis of Global Burden of Disease Study 2019.BMC Med. 2023 Jun 26;21(1):222. doi: 10.1186/s12916-023-02925-4. BMC Med. 2023. PMID: 37365627 Free PMC article.
-
VEGF-A cis-located SNPs on human chromosome 6 associated with VEGF-A plasma levels and survival in a coronary disease cohort.BMC Cardiovasc Disord. 2025 Apr 17;25(1):290. doi: 10.1186/s12872-025-04751-3. BMC Cardiovasc Disord. 2025. PMID: 40247170 Free PMC article.
-
The Chilean burden of disability-adjusted life years due to cardiovascular diseases: Results from the Global Burden of Disease Study 2021.PLoS One. 2025 Jun 18;20(6):e0325519. doi: 10.1371/journal.pone.0325519. eCollection 2025. PLoS One. 2025. PMID: 40531858 Free PMC article.
-
Global Healthspan-Lifespan Gaps Among 183 World Health Organization Member States.JAMA Netw Open. 2024 Dec 2;7(12):e2450241. doi: 10.1001/jamanetworkopen.2024.50241. JAMA Netw Open. 2024. PMID: 39661386 Free PMC article.
References
-
- Institute of Health Metrics and Evaluation. New Zealand (country profile). (Accessed 15 January 2022). https://www.healthdata.org/new-zealand.
-
- Institute for health Metrics and Evaluation. Global Burden of Disease (GBD) Results Tool. (Accessed 15 January 2022). http://ghdx.healthdata.org/gbd-results-tool
-
- Grey C, Jackson R, Wells S, Wu B, Poppe K, Harwood M, et al. Trends in ischaemic heart disease: patterns of hospitalisation and mortality rates differ by ethnicity (ANZACS-QI 21) N Z Med J. 2018;131(1478):21–31. - PubMed
-
- Selak V, Poppe K, Grey C, Mehta S, Winter-Smith J, Jackson R, et al. Ethnic differences in cardiovascular risk profiles among 475,241 adults in primary care in Aotearoa, New Zealand. N Z Med J. 2020;133(1521):14–27. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
