

Medical insurance payment schemes and patient medical expenses: a cross-sectional study of lung cancer patients in urban China
- PMID: 36703175
- PMCID: PMC9881291
- DOI: 10.1186/s12913-023-09078-3
Medical insurance payment schemes and patient medical expenses: a cross-sectional study of lung cancer patients in urban China
Abstract
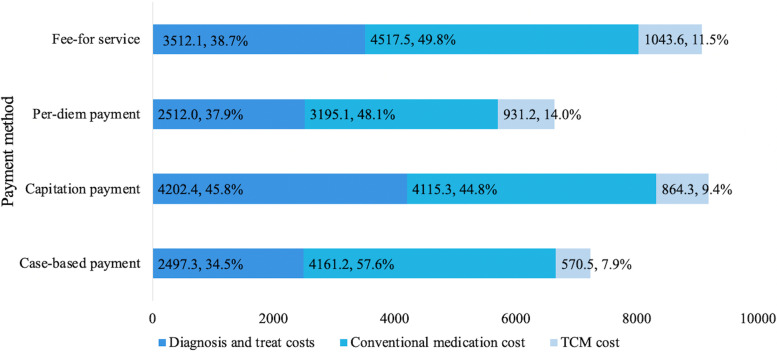
Background: As the main cause of cancer death, lung cancer imposes seriously health and economic burdens on individuals, families, and the health system. In China, there is no national study analyzing the hospitalization expenditures of different payment methods by lung cancer inpatients. Based on the 2010-2016 database of insured urban resident lung cancer inpatients from the China Medical Insurance Research Association (CHIRA), this paper aims to investigate the characteristics and cost of hospitalized lung cancer patient, to examine the differences in hospital expenses and patient out-of-pocket (OOP) expenses under four medical insurance payment methods: fee-for-service (FFS), per-diem payments, capitation payments (CAP) and case-based payments, and to explore the medical insurance payment method that can be conducive to controlling the cost of lung cancer.
Method: This is a 2010-2016, 7-year cross-sectional study. CHIRA data are not available to researchers after 2016. The Medical Insurance Database of CHIRA was screened using the international disease classification system to yield 28,200 inpatients diagnosed with lung cancer (ICD-10: C34, C34.0, C34.1, C34.2, C34.3, C34.8, C34.9). The study includes descriptive analysis and regression analysis based on generalized linear models (GLM).
Results: The average patient age was 63.4 years and the average length of hospital stay (ALOS) was 14.2 day; 60.7% of patients were from tertiary hospitals; and 45% were insured by FFS. The per-diem payment had the lowest hospital expenses (RMB7496.00/US$1176.87), while CAP had the lowest OOP expenses (RMB1328.18/US$208.52). Compared with FFS hospital expenses, per-diem was 21.3% lower (95% CI = -0.265, -0.215) and case-based payment was 8.4% lower (95% CI = -0.151, -0.024). Compared with the FFS, OOP expenses, per-diem payments were 9.2% lower (95% CI = -0.130, -0.063) and CAP was 15.1% lower (95% CI = -0.151, -0.024).
Conclusion: For lung cancer patients, per-diem payment generated the lowest hospital expenses, while CAP meant patients bore the lowest OOP costs. Policy makers are suggested to give priority to case-based payments to achieve a tripartite balance among medical insurers, hospitals, and insured members. We also recommend future studies comparing the disparities of various diseases for the cause of different medical insurance schemes.
Keywords: Hospital expenses; Lung cancer; Out-of-pocket expenses; Payment method.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Managing Urban Stroke Health Expenditures in China: Role of Payment Method and Hospital Level.Int J Health Policy Manag. 2022 Dec 6;11(11):2698-2706. doi: 10.34172/ijhpm.2022.5117. Epub 2022 Feb 22. Int J Health Policy Manag. 2022. PMID: 35219287 Free PMC article.
-
Effect of health insurance on direct hospitalisation costs for in-patients with ischaemic stroke in China.Aust Health Rev. 2018 Feb;42(1):39-44. doi: 10.1071/AH16056. Aust Health Rev. 2018. PMID: 28263706
-
How provider payment methods affect health expenditure of depressive patients? Empirical study from national claims data in China from 2013 to 2017.J Affect Disord. 2024 Apr 1;350:286-294. doi: 10.1016/j.jad.2024.01.100. Epub 2024 Jan 12. J Affect Disord. 2024. PMID: 38220107
-
The impact of diagnosis-related group-based medical insurance payment model on the prognosis and nursing care of patients undergoing composite trabeculectomy: a retrospective cohort study.Front Public Health. 2025 May 21;13:1518546. doi: 10.3389/fpubh.2025.1518546. eCollection 2025. Front Public Health. 2025. PMID: 40469599 Free PMC article. Review.
-
Costs of inpatient care and out-of-pocket payments for COVID-19 patients: A systematic review.PLoS One. 2023 Sep 20;18(9):e0283651. doi: 10.1371/journal.pone.0283651. eCollection 2023. PLoS One. 2023. PMID: 37729207 Free PMC article.
Cited by
-
Climate risks, multi-tier medical insurance systems, and health inequality: evidence from China's middle-aged and elderly populations.BMC Health Serv Res. 2025 Apr 1;25(1):481. doi: 10.1186/s12913-025-12648-2. BMC Health Serv Res. 2025. PMID: 40170171 Free PMC article.
-
Does basic medical insurance promote public health? Evidence from China family panel study.Front Public Health. 2023 Dec 14;11:1269277. doi: 10.3389/fpubh.2023.1269277. eCollection 2023. Front Public Health. 2023. PMID: 38162604 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
