

The genomic landscape of rare disorders in the Middle East
- PMID: 36703223
- PMCID: PMC9881316
- DOI: 10.1186/s13073-023-01157-8
The genomic landscape of rare disorders in the Middle East
Abstract
Background: Rare diseases collectively impose a significant burden on healthcare systems, especially in underserved regions, like the Middle East, which lack access to genomic diagnostic services and the associated personalized management plans.
Methods: We established a clinical genomics and genetic counseling facility, within a multidisciplinary tertiary pediatric center, in the United Arab Emirates to locally diagnose and manage patients with rare diseases. Clinical genomic investigations included exome-based sequencing, chromosomal microarrays, and/or targeted testing. We assessed the diagnostic yield and implications for clinical management among this population. Variables were compared using the Fisher exact test. Tests were 2-tailed, and P < .05 was considered statistically significant.
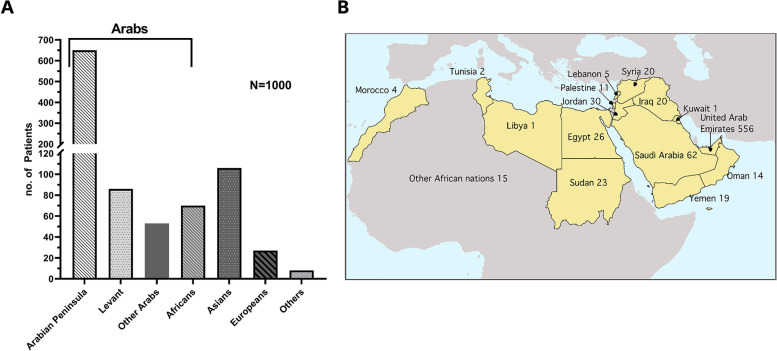
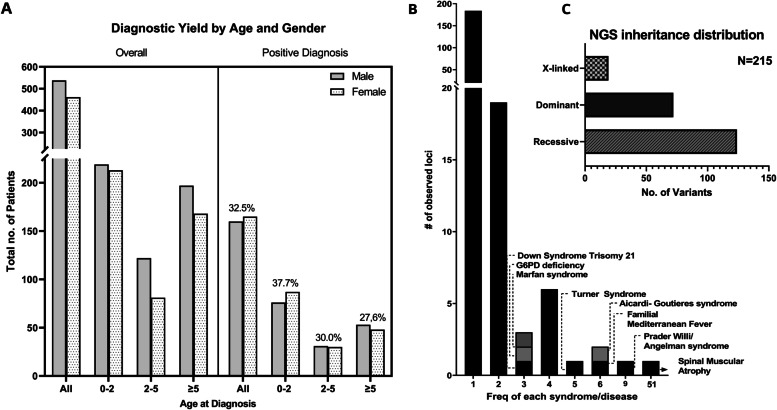
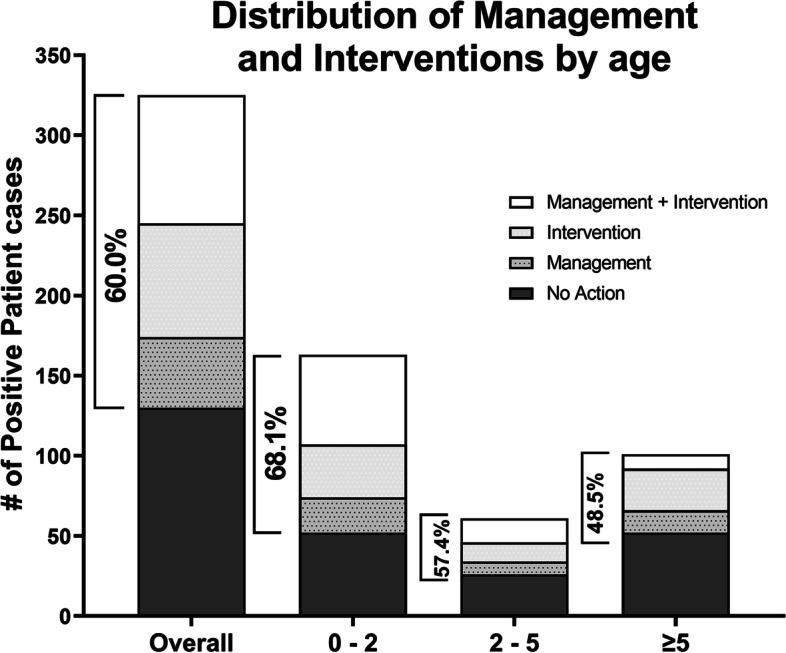
Results: We present data on 1000 patients with rare diseases (46.2% females; average age, 4.6 years) representing 47 countries primarily from the Arabian Peninsula, the Levant, Africa, and Asia. The cumulative diagnostic yield was 32.5% (95% CI, 29.7-35.5%) and was higher for genomic sequencing-based testing than chromosomal microarrays (37.9% versus 17.2%, P = 0.0001) across all indications, consistent with the higher burden of single gene disorders. Of the 221 Mendelian disorders identified in this cohort, the majority (N = 184) were encountered only once, and those with recessive inheritance accounted for ~ 62% of sequencing diagnoses. Of patients with positive genetic findings (N = 325), 67.7% were less than 5 years of age, and 60% were offered modified management and/or intervention plans. Interestingly, 24% of patients with positive genetic findings received delayed diagnoses (average age, 12.4 years; range 7-37 years), most likely due to a lack of access to genomic investigations in this region. One such genetic finding ended a 15-year-long diagnostic odyssey, leading to a life-threatening diagnosis in one patient, who was then successfully treated using an experimental allogenic bone marrow transplant. Finally, we present cases with candidate genes within regions of homozygosity, likely underlying novel recessive disorders.
Conclusions: Early access to genomic diagnostics for patients with suspected rare disorders in the Middle East is likely to improve clinical outcomes while driving gene discovery in this genetically underrepresented population.
Keywords: Clinical utility; Diagnostic yield; Genomics; Middle East; Rare diseases; Whole-exome sequencing.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Rare disease facts - global genes. Accessed August 22, 2022. https://globalgenes.org/rare-disease-facts/.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
