

Rescue stenting after the failure of mechanical thrombectomy to treat acute intracranial atherosclerotic occlusion
- PMID: 36703624
- PMCID: PMC9873241
- DOI: 10.3389/fneur.2022.1001496
Rescue stenting after the failure of mechanical thrombectomy to treat acute intracranial atherosclerotic occlusion
Abstract
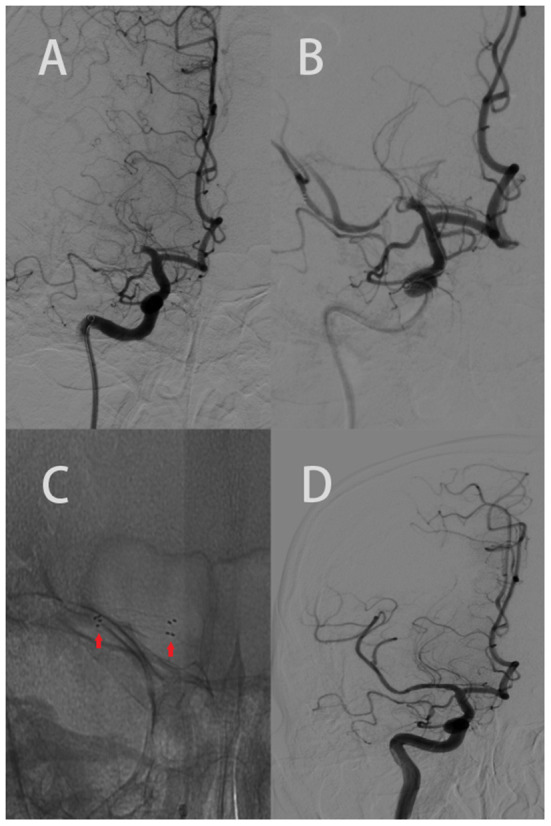
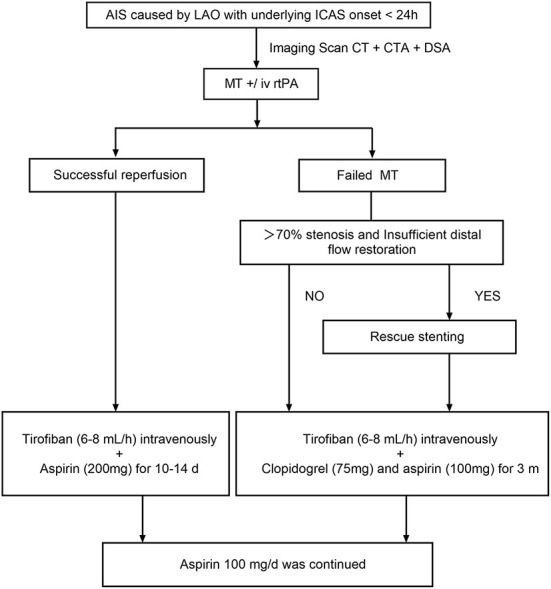
Background: Acute ischemic stroke (AIS) with intracranial large vessel occlusion (LVO) is refractory to reperfusion because of the underlying intracranial atherosclerosis (ICAS), and this condition often requires salvage methods such as balloon angioplasty and rescue stenting (RS). In this study, we investigated the short-term outcomes of RS after failed mechanical thrombectomy (MT) for the treatment of acute intracranial atherosclerotic occlusion.
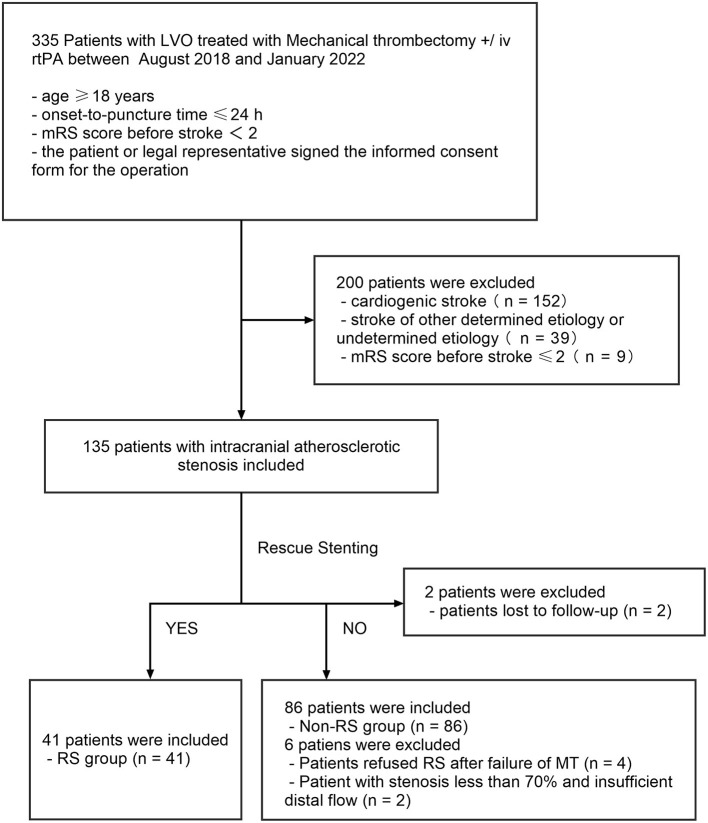
Methods: We retrospectively evaluated the clinical data of 127 patients who underwent MT for acute intracranial atherosclerotic occlusion in our hospital between August 2018 and January 2022. The degree of recanalization was evaluated immediately after the treatment by Modified Thrombolysis in Cerebral Infarction (mTICI). The modified Rankin Scale (mRS) was used 90 days after treatment to evaluate the neurological functions. In addition, the incidence of symptomatic intracranial hemorrhage (sICH) and postoperative mortality within 90 days of treatment were calculated.
Results: Among the 127 patients, 86 patients (67.7%) had revascularization (mTICI 2b-3) immediately after MT (non-RS group), and RS was performed in 41 patients (32.3%) after MT failure (RS group). No difference in the sICH rate was observed between the two groups (17.1 vs. 16.3%, p = 0.91). There was a slightly higher mortality rate in the RS group (14.6 vs. 12.8%, p = 0.71); however, the difference was not significant. There was no difference in the proportion of patients in the RS and non-RS groups who had a 90-day mRS score of 0-2 (48.8 vs. 52.3%, p = 0.76).
Conclusions: Rescue stenting after MT failure might be a feasible rescue modality for treating acute intracranial atherosclerotic occlusion.
Keywords: acute ischemic stroke; intracranial atherosclerosis; mechanical thrombectomy; rescue stenting; symptomatic intracerebral hemorrhage.
Copyright © 2023 Guo, Jin, Xu, Huang, Shi and Geng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Stenting and Angioplasty in Neurothrombectomy: Matched Analysis of Rescue Intracranial Stenting Versus Failed Thrombectomy.Stroke. 2022 Sep;53(9):2779-2788. doi: 10.1161/STROKEAHA.121.038248. Epub 2022 Jun 30. Stroke. 2022. PMID: 35770672
-
Emergency Angioplasty or Stenting for Stroke Patients with Intracranial Atherosclerotic Large Vessel Occlusion.J Atheroscler Thromb. 2023 Feb 1;30(2):160-169. doi: 10.5551/jat.63381. Epub 2022 Apr 22. J Atheroscler Thromb. 2023. PMID: 35466122 Free PMC article.
-
Intracranial Stenting as Rescue Therapy After Failure of Mechanical Thrombectomy for Basilar Artery Occlusion: Data From the ANGEL-ACT Registry.Front Neurol. 2021 Sep 30;12:739213. doi: 10.3389/fneur.2021.739213. eCollection 2021. Front Neurol. 2021. PMID: 34659098 Free PMC article.
-
Rescue Intracranial Stenting After Failed Mechanical Thrombectomy for Acute Ischemic Stroke: A Systematic Review and Meta-Analysis.World Neurosurg. 2019 Dec;132:e235-e245. doi: 10.1016/j.wneu.2019.08.192. Epub 2019 Sep 5. World Neurosurg. 2019. PMID: 31493593
-
Rescue intracranial stenting for acute ischemic stroke after the failure of mechanical thrombectomy: A systematic review, meta-analysis, and trial sequential analysis.Front Neurol. 2023 Jan 25;14:1023089. doi: 10.3389/fneur.2023.1023089. eCollection 2023. Front Neurol. 2023. PMID: 36761342 Free PMC article.
Cited by
-
Hypoperfusion Intensity Ratio Less Than 0.4 Is Associated with Favorable Outcomes in Unsuccessfully Reperfused Acute Ischemic Stroke with Large-Vessel Occlusion.AJNR Am J Neuroradiol. 2025 Mar 4;46(3):483-488. doi: 10.3174/ajnr.A8518. AJNR Am J Neuroradiol. 2025. PMID: 39979027
-
Determinants of day-1 stent patency following rescue intracranial stenting in failed intracranial thrombectomy.Interv Neuroradiol. 2025 May 21:15910199251339900. doi: 10.1177/15910199251339900. Online ahead of print. Interv Neuroradiol. 2025. PMID: 40398455 Free PMC article.
-
Mechanical thrombectomy for AIS from large vessel occlusion - current trends and future perspectives.Ann Med Surg (Lond). 2023 Oct 4;85(12):6021-6028. doi: 10.1097/MS9.0000000000001385. eCollection 2023 Dec. Ann Med Surg (Lond). 2023. PMID: 38098569 Free PMC article. Review.
References
-
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. . Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of a cute ischemic stroke: a guideline for healthcare professionals from the American heart association/American stroke association. Stroke. (2019) 50:e344–418. 10.1161/STR.0000000000000211 - DOI - PubMed
LinkOut - more resources
Full Text Sources