

Systemic inflammation response index as a prognostic predictor in patients with acute ischemic stroke: A propensity score matching analysis
- PMID: 36703636
- PMCID: PMC9871574
- DOI: 10.3389/fneur.2022.1049241
Systemic inflammation response index as a prognostic predictor in patients with acute ischemic stroke: A propensity score matching analysis
Abstract
Background: Acute ischemic stroke (AIS), the most common type of stroke, is a major cause of morbidity and mortality worldwide. A growing number of studies have demonstrated that inflammation is a critical mechanism in AIS. Being an easily available and effective inflammatory marker, the systemic inflammation response index (SIRI) shows a high association with mortality in patients with cancer and intracerebral hemorrhage. In this study, we evaluated the potential prognostic role of SIRI in critically ill patients with AIS.
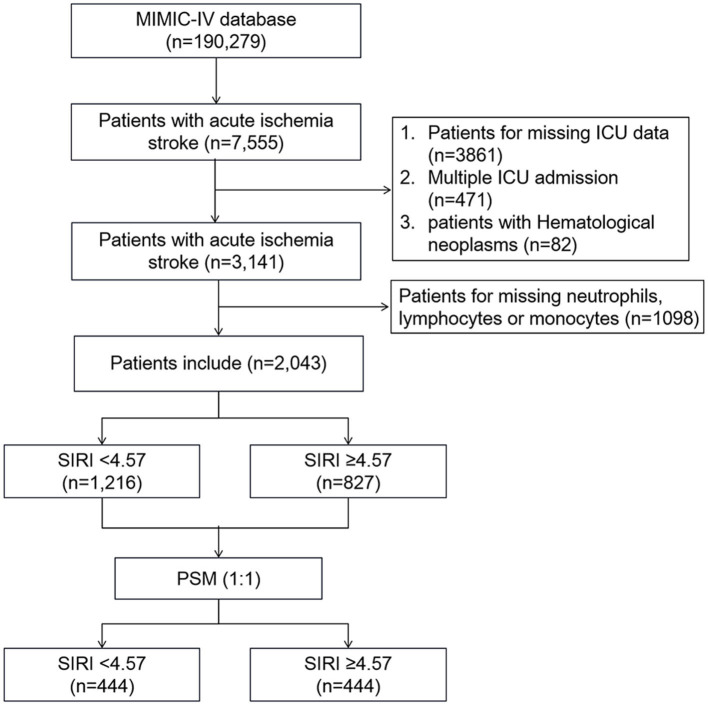
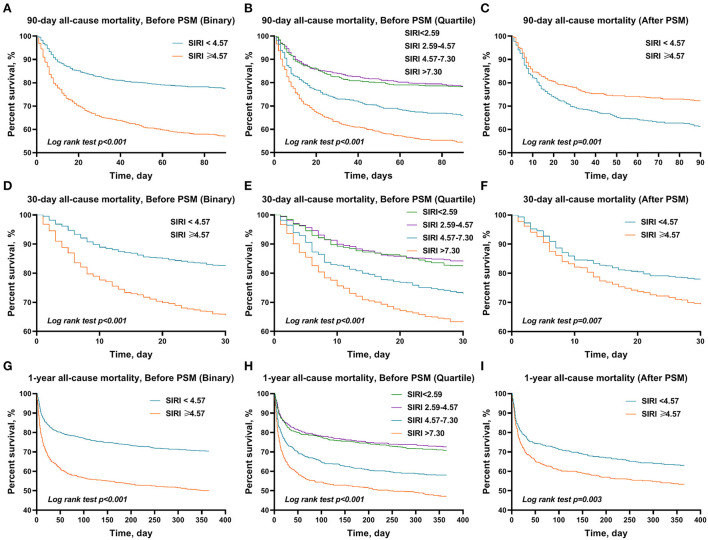
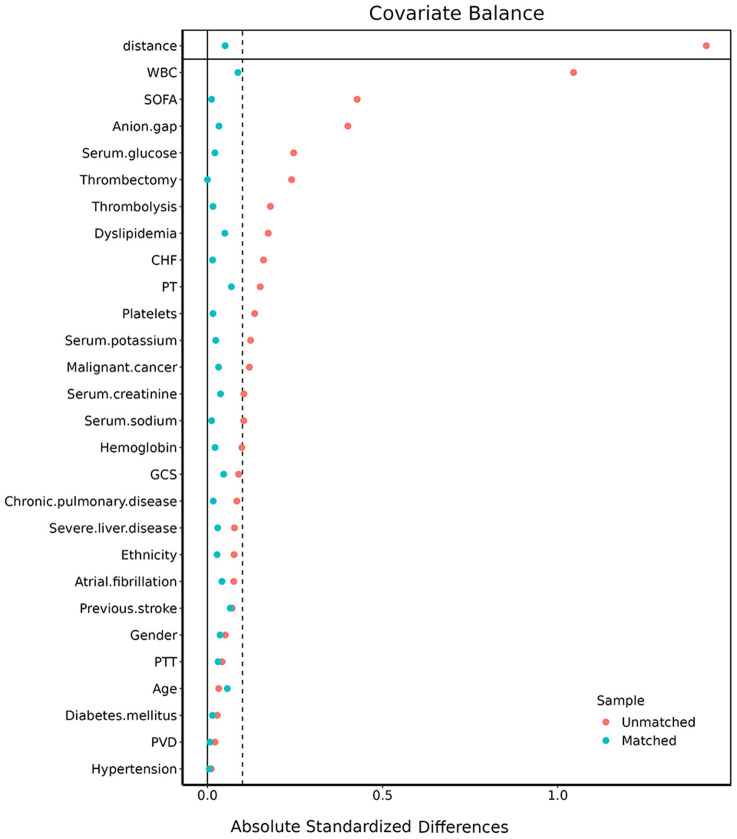
Methods: Clinic data were extracted from the Medical Information Mart data for the Intensive Care IV (MIMIC-IV) database. The optimal cutoff value of SIRI was determined by X-tile software. The primary outcome was the 90-day all-cause mortality, and the secondary outcomes were 30-day and 1-year all-cause mortality of patients with AIS. Cox proportional hazards regression analyses were used to assess the association between SIRI levels and all-cause mortality, and survival curves were estimated using the Kaplan-Meier method. Furthermore, a 1:1 propensity score matching (PSM) method was performed to balance the influence of potential confounding factors.
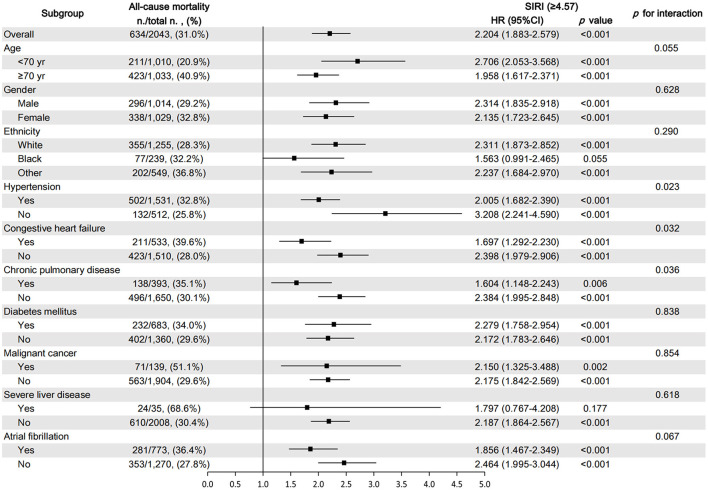
Results: A total of 2,043 patients were included in our study. X-tile software indicated that the optimal cutoff value of the SIRI for 90-day mortality was 4.57. After PSM, 444 pairs of score-matched patients were generated. Cox proportional hazard model showed that after adjusting for possible confounders, high SIRI level (≥4.57) was independently associated with the 90-day all-cause mortality in the cohort before PSM (HR = 1.56, 95% CI: 1.30-1.89, p < 0.001) and the PSM subset (HR = 1.47, 95% CI: 1.16-1.86, p = 0.001). The survival curves showed that patients with SIRI ≥4.57 had a significantly lower 90-day survival rate in the cohort before PSM (56.7 vs. 77.3%, p < 0.001) and the PSM subset (61.0 vs. 71.8%, p = 0.001). Consistently, AIS patients with high SIRI levels (≥4.57) presented a significantly high risk of 30-day and 1-year all-cause mortality before and after PSM.
Conclusion: A higher SIRI (≥4.57) was associated with a higher risk of 90-day, 30-day, and 1-year mortality and was an independent risk factor of mortality in patients with acute ischemic stroke.
Keywords: ischemic stroke; mortality; predictor; propensity score matching (PSM); systemic inflammation response index.
Copyright © 2023 Dang, Mao, Wang, Sha, Lu, Cong, Meng and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Association between a four-parameter inflammatory index and all-cause mortality in critical ill patients with non-traumatic subarachnoid hemorrhage: a retrospective analysis of the MIMIC-IV database (2012-2019).Front Immunol. 2023 Oct 23;14:1235266. doi: 10.3389/fimmu.2023.1235266. eCollection 2023. Front Immunol. 2023. PMID: 37936706 Free PMC article.
-
The predictive role of systemic inflammation response index in the prognosis of traumatic brain injury: A propensity score matching study.Front Neurol. 2022 Nov 2;13:995925. doi: 10.3389/fneur.2022.995925. eCollection 2022. Front Neurol. 2022. PMID: 36408504 Free PMC article.
-
Systemic inflammation response index as a predictor of 3-month functional outcomes in acute ischemic stroke patients following intravenous thrombolysis.Neuroscience. 2025 Jun 7;576:234-240. doi: 10.1016/j.neuroscience.2025.04.043. Epub 2025 Apr 26. Neuroscience. 2025. PMID: 40294845
-
Systemic inflammation response index as a clinical outcome evaluating tool and prognostic indicator for hospitalized stroke patients: a systematic review and meta-analysis.Eur J Med Res. 2023 Nov 1;28(1):474. doi: 10.1186/s40001-023-01446-3. Eur J Med Res. 2023. PMID: 37915088 Free PMC article.
-
Association between Systemic Immune-Inflammation Index and Systemic Inflammation Response Index and Outcomes of Acute Ischemic Stroke: A Systematic Review and Meta-Analysis.Ann Indian Acad Neurol. 2023 Sep-Oct;26(5):655-662. doi: 10.4103/aian.aian_85_23. Epub 2023 Jul 20. Ann Indian Acad Neurol. 2023. PMID: 38022472 Free PMC article. Review.
Cited by
-
Body fluids biomarkers associated with prognosis of acute ischemic stroke: progress and prospects.Future Sci OA. 2024 May 20;10(1):FSO931. doi: 10.2144/fsoa-2023-0142. eCollection 2024. Future Sci OA. 2024. PMID: 38817358 Free PMC article. Review.
-
Fibromyalgia: Chronic Pain Due to a Blood Dysfunction?Int J Mol Sci. 2025 Apr 27;26(9):4153. doi: 10.3390/ijms26094153. Int J Mol Sci. 2025. PMID: 40362392 Free PMC article. Review.
-
The Dual Role of Autophagy in Postischemic Brain Neurodegeneration of Alzheimer's Disease Proteinopathy.Int J Mol Sci. 2023 Sep 7;24(18):13793. doi: 10.3390/ijms241813793. Int J Mol Sci. 2023. PMID: 37762096 Free PMC article. Review.
-
Analysis of the Associations of Measurements of Body Composition and Inflammatory Factors with Cardiovascular Disease and Its Comorbidities in a Community-Based Study.Biomedicines. 2024 May 11;12(5):1066. doi: 10.3390/biomedicines12051066. Biomedicines. 2024. PMID: 38791028 Free PMC article.
-
Development and Validation of the Systemic Inflammatory Response Index-Based Nomogram for Predicting Short-Term Adverse Events in Patients With Acute Uncomplicated Type B Aortic Intramural Hematoma.J Inflamm Res. 2025 Jan 28;18:1303-1316. doi: 10.2147/JIR.S496007. eCollection 2025. J Inflamm Res. 2025. PMID: 39897519 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous