

Impact of mouse model tumor implantation site on acquired resistance to anti-PD-1 immune checkpoint therapy
- PMID: 36703964
- PMCID: PMC9872099
- DOI: 10.3389/fimmu.2022.1011943
Impact of mouse model tumor implantation site on acquired resistance to anti-PD-1 immune checkpoint therapy
Abstract
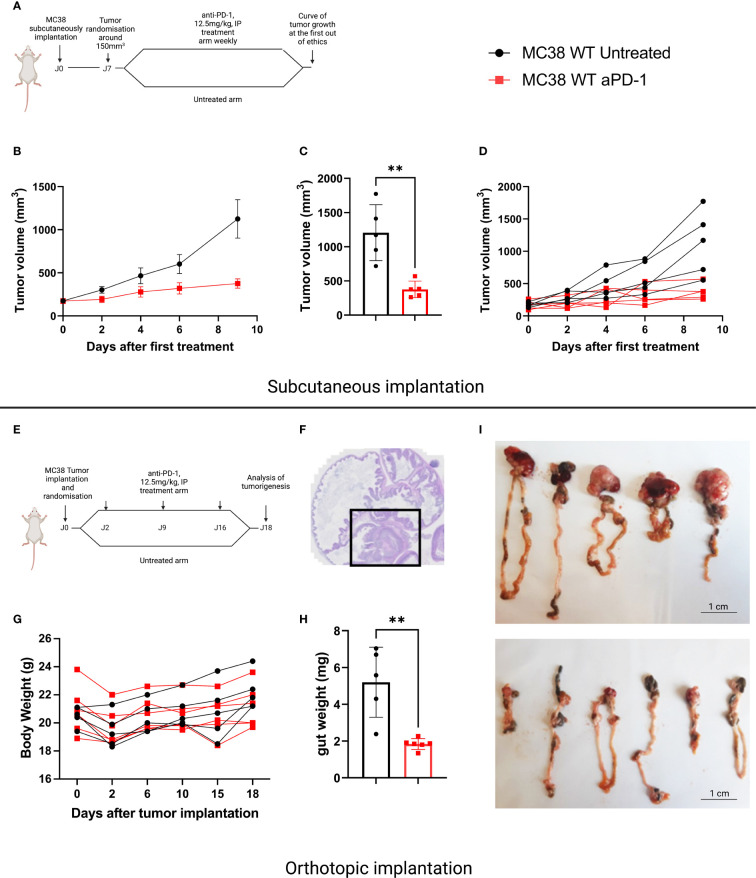
Introduction: The use of tumor subcutaneous (SC) implantations rather than orthotopic sites is likely to induce a significant bias, in particular, in the field of immunotherapy.
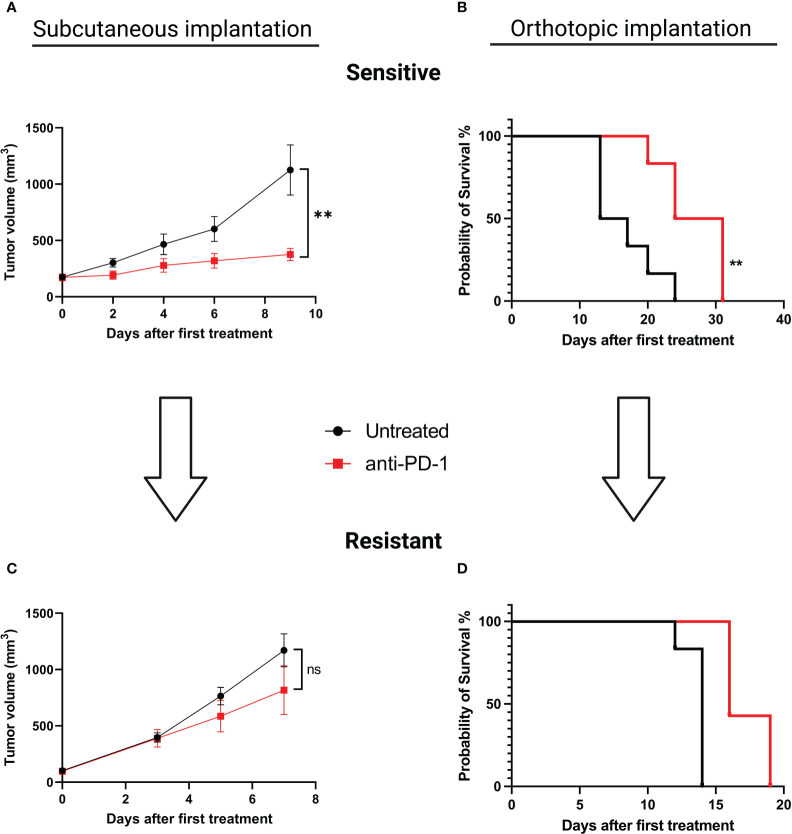
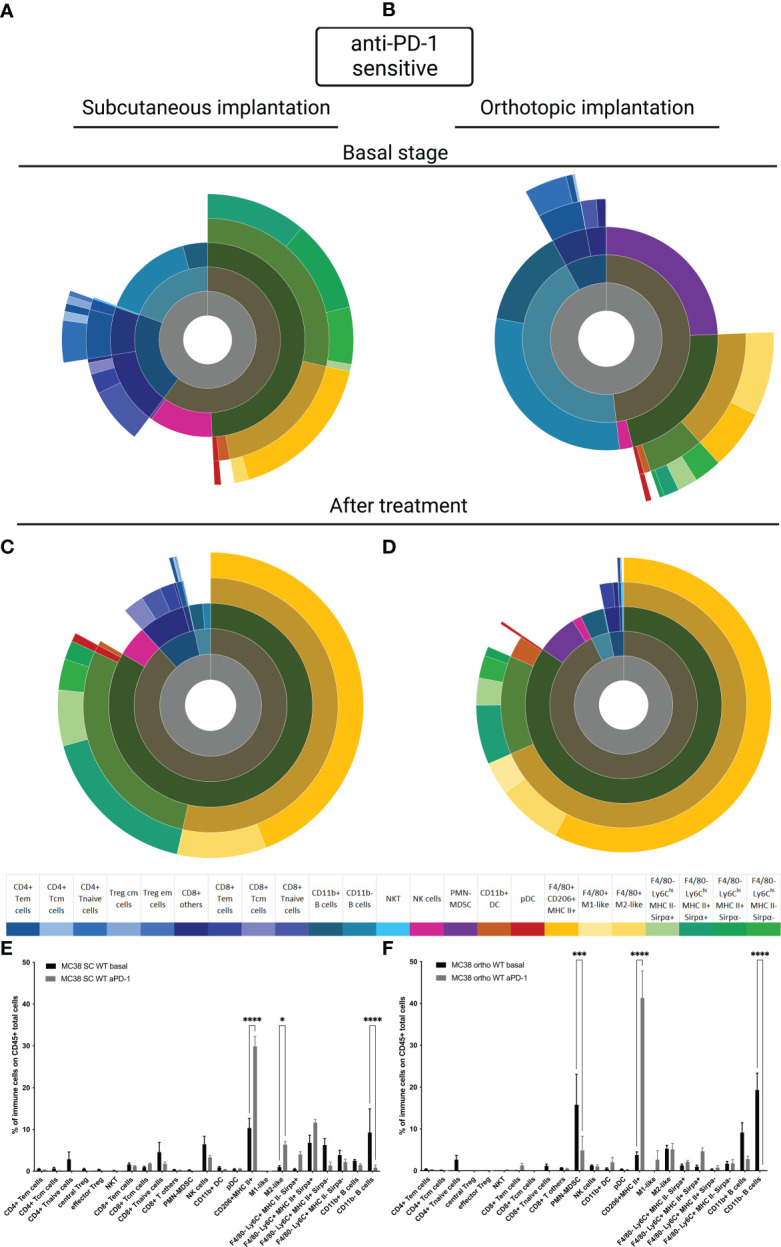
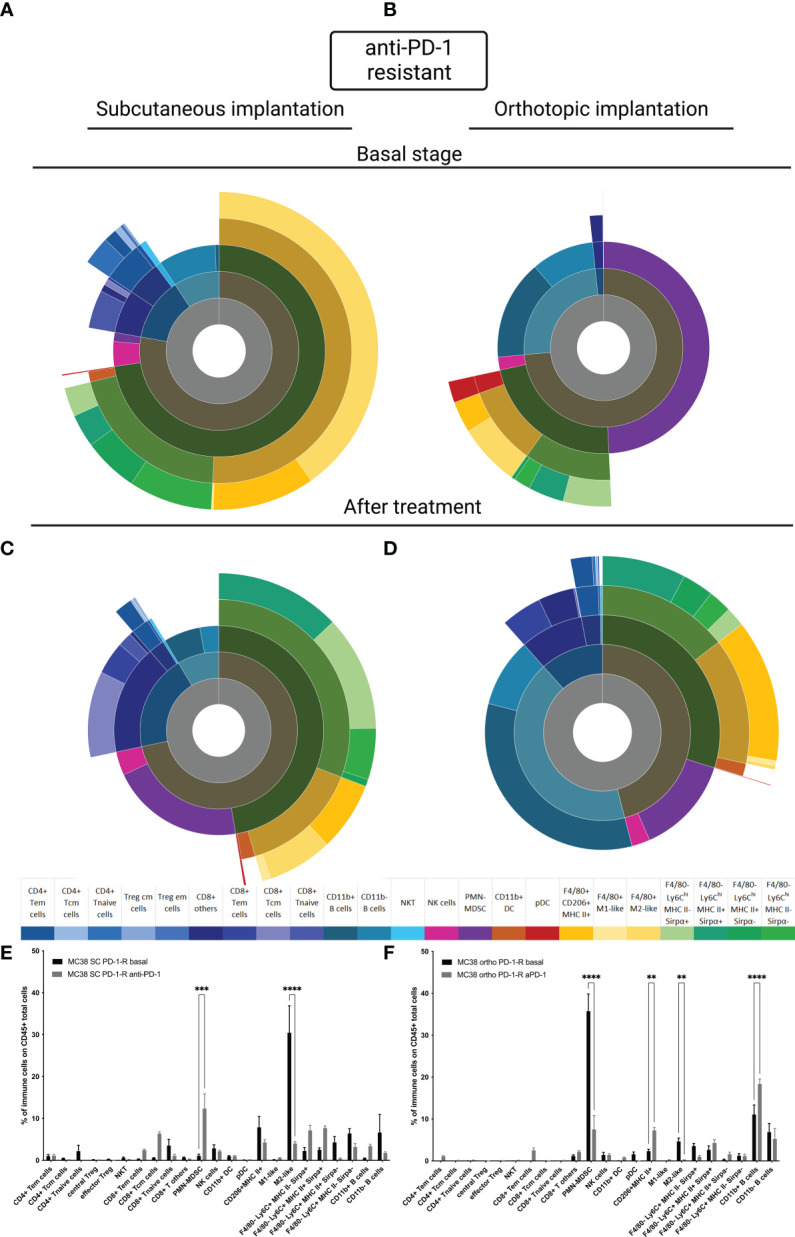
Methods: In this study, we developed and characterized MC38 models, implanted subcutaneously and orthotopically, which were either sensitive or rendered resistant to anti-PD1 therapy. We characterized the tumor immune infiltrate by flow cytometry at baseline and after treatment.
Results and discussion: Our results demonstrate several differences between SC and orthotopic models at basal state, which tend to become similar after therapy. These results emphasize the need to take into account tumor implantation sites when performing preclinical studies with immunotherapeutic agents.
Keywords: orthotopic; MC38; anti-PD-1; preclinical model; subcutaneous.
Copyright © 2023 Denis, Mathé, Micoud, Choffour, Grasselly, Matera and Dumontet.
Conflict of interest statement
MD, DM and P-AC were employed by Antineo, a CRO offering preclinical models in oncopharmacology. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Synergy between Toxoplasma gondii type I ΔGRA17 immunotherapy and PD-L1 checkpoint inhibition triggers the regression of targeted and distal tumors.J Immunother Cancer. 2021 Nov;9(11):e002970. doi: 10.1136/jitc-2021-002970. J Immunother Cancer. 2021. PMID: 34725213 Free PMC article.
-
The Tumor Microenvironment Regulates Sensitivity of Murine Lung Tumors to PD-1/PD-L1 Antibody Blockade.Cancer Immunol Res. 2017 Sep;5(9):767-777. doi: 10.1158/2326-6066.CIR-16-0365. Epub 2017 Aug 17. Cancer Immunol Res. 2017. PMID: 28819064 Free PMC article.
-
In situ immunogenic clearance induced by a combination of photodynamic therapy and rho-kinase inhibition sensitizes immune checkpoint blockade response to elicit systemic antitumor immunity against intraocular melanoma and its metastasis.J Immunother Cancer. 2021 Jan;9(1):e001481. doi: 10.1136/jitc-2020-001481. J Immunother Cancer. 2021. PMID: 33479026 Free PMC article.
-
Resistance mechanisms to checkpoint inhibitors.Curr Opin Immunol. 2021 Apr;69:47-55. doi: 10.1016/j.coi.2021.02.001. Epub 2021 Mar 3. Curr Opin Immunol. 2021. PMID: 33676271 Review.
-
Advances in the Study of Antitumour Immunotherapy for Newcastle Disease Virus.Int J Med Sci. 2021 Mar 30;18(11):2294-2302. doi: 10.7150/ijms.59185. eCollection 2021. Int J Med Sci. 2021. PMID: 33967605 Free PMC article. Review.
Cited by
-
Aerobic exercise training mitigates tumor growth and cancer-induced splenomegaly through modulation of non-platelet platelet factor 4 expression.Sci Rep. 2023 Dec 11;13(1):21970. doi: 10.1038/s41598-023-47217-2. Sci Rep. 2023. PMID: 38081853 Free PMC article.
-
Spatiotemporal commonality of the TCR repertoire in a T-cell memory murine model and in metastatic human colorectal cancer.Cancer Immunol Immunother. 2023 Sep;72(9):2971-2989. doi: 10.1007/s00262-023-03473-9. Epub 2023 Jun 4. Cancer Immunol Immunother. 2023. PMID: 37270735 Free PMC article.
-
Engagement of CD99 Activates Distinct Programs in Ewing Sarcoma and Macrophages.Cancer Immunol Res. 2024 Feb 2;12(2):247-260. doi: 10.1158/2326-6066.CIR-23-0440. Cancer Immunol Res. 2024. PMID: 38051221 Free PMC article.
-
Engineered GM-CSF polarizes protumorigenic tumor-associated macrophages to an antitumorigenic phenotype and potently synergizes with IL-12 immunotherapy.J Immunother Cancer. 2024 Dec 22;12(12):e009541. doi: 10.1136/jitc-2024-009541. J Immunother Cancer. 2024. PMID: 39794939 Free PMC article.
-
Therapeutic efficacy of plant-produced Nivolumab in transgenic C57BL/6-hPD-1 mouse implanted with MC38 colon cancer.Biotechnol Rep (Amst). 2023 Mar 28;38:e00794. doi: 10.1016/j.btre.2023.e00794. eCollection 2023 Jun. Biotechnol Rep (Amst). 2023. PMID: 37064962 Free PMC article.
References
-
- Balar AV, Galsky MD, Rosenberg JE, Powles T, Petrylak DP, Bellmunt J, et al. . Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: A single-arm, multicentre, phase 2 trial. Lancet (2017) 389:67–76. doi: 10.1016/S0140-6736(16)32455-2 - DOI - PMC - PubMed
-
- Cella D, Grünwald V, Escudier B, Hammers HJ, George S, Nathan P, et al. . Patient-reported outcomes of patients with advanced renal cell carcinoma treated with nivolumab plus ipilimumab versus sunitinib (CheckMate 214): a randomised, phase 3 trial. Lancet Oncol (2019) 20:297–310. doi: 10.1016/S1470-2045(18)30778-2 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical