

A mixed-method evaluation of the relationship between Oxford classification scores and longitudinal changes in proteinuria in patients with immunoglobulin A nephropathy
- PMID: 36704031
- PMCID: PMC9871483
- DOI: 10.3389/fendo.2022.890900
A mixed-method evaluation of the relationship between Oxford classification scores and longitudinal changes in proteinuria in patients with immunoglobulin A nephropathy
Abstract
Introduction: This study aimed to investigate the relationship between Oxford Classification scores and longitudinal changes in proteinuria in patients with immunoglobulin A nephropathy (IgAN).
Methods: The study was a single-center retrospective cohort study involving 358 patients with primary IgAN who were treated at the Shenzhen Second People's Hospital, China, between January 2011 and May 2021. Multivariate linear regression and generalized additive mixed models (GAMMs), adjusted for traditional risk confounders, were used to evaluate the correlation between scores for mesangial hypercellularity (M), endocapillary hypercellularity (E), segmental glomerulosclerosis (S), tubular atrophy/interstitial fibrosis (T), and crescents (C) (known as the Oxford Classification MEST-C score system), with proteinuria/creatinine ratio (PCR) at the time of renal biopsy and longitudinal changes in PCR, respectively.
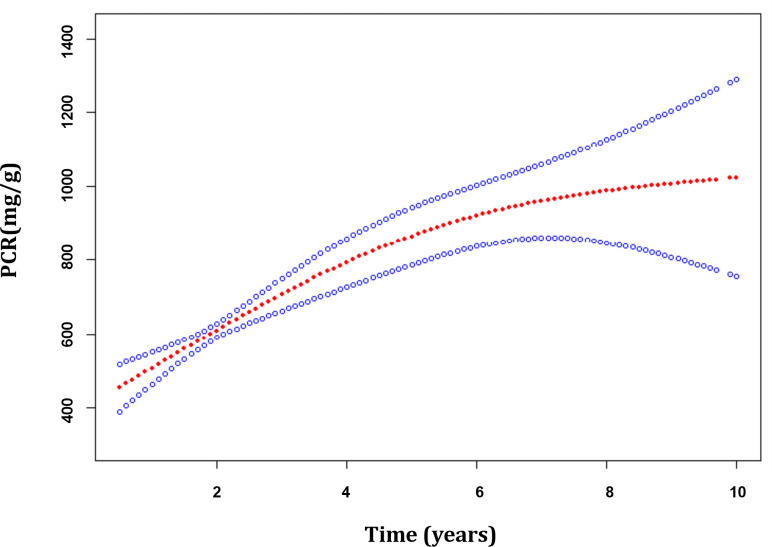
Results: The median PCR was 1061 mg/g, and it increased on average by 68.82 mg/g per year in these patients. Among patients with renal insufficiency, compared with patients without relative lesions, those with E present (E1) (1153.44; 95% confidence interval [CI], 188.99-2117.89 mg/g) and C > 0 (C1/2) (1063.58; 95% CI, 185.25-1941.90 mg/g) were associated with increased PCR levels at the time of renal biopsy. What's more, S present (S1) (194.96; 95% CI, 54.50-335.43 mg/g per year) was associated with the fastest PCR increase; C > 0 (C1/2) (147.59; 95% CI, 8.32-286.86 mg/g per year) and T >25% (T1/2) (77.04; 95% CI, 7.18-146.89 mg/g per year), were also correlated with a faster PCR increase. In patients with normal kidney function, associations between S1 (55.46; 95% CI, 8.93-101.99 mg/g per year) and E1 (94.02; 95% CI, 21.47-166.58 mg/g per year) and PCR change could be observed. Additionally, in patients with overweight/obesity, S1 (156.09; 95% CI, 52.41-259.77 mg/g per year), E1 (143.34; 95% CI, 35.30-251.38 mg/g per year), T1/2 (116.04; 95% CI, 22.58-209.51 mg/g per year), as well as C1/2 (134.03; 95% CI, 41.73-226.32 mg/g per year) were associated with noticeably quicker PCR increase.
Conclusions: Overall, E1 and C1/2 were independently associated with raised proteinuria levels at the time of renal biopsy, and S1, E1, T1/2, C1/2 were independently associated with a longitudinal increase in proteinuria in the patients with IgAN, especially in those with renal insufficiency or overweight/obesity, suggesting that currently available treatments might not be satisfactory, and weight control might be beneficial. Individual therapy development might benefit from the use of the Oxford Classification system.
Keywords: IgA nephropathy; Oxford classification; mixed methods; proteinuria/creatinine ratio; renal function.
Copyright © 2023 Xu, Guo, Cao, Xu, Liao, Chen, Song, Chen, Guan, Tang, Xiang, Chen and Wan.
Conflict of interest statement
Author X-LC is employed by Empower U, X&Y solutions Inc. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
The Association of the Oxford Classification Score with Longitudinal Estimated Glomerular Filtration Rate Decline in Patients with Immunoglobulin A Nephropathy: A Mixed-Method Study.Int J Gen Med. 2021 Jun 18;14:2655-2663. doi: 10.2147/IJGM.S313333. eCollection 2021. Int J Gen Med. 2021. PMID: 34177274 Free PMC article.
-
Is it possible to predict parameters of the Oxford classification of primary IgA Nephropathy from clinical laboratory data? Focus on the role of segmental glomerulosclerosis subtypes.Pathol Res Pract. 2019 Oct;215(10):152533. doi: 10.1016/j.prp.2019.152533. Epub 2019 Jul 12. Pathol Res Pract. 2019. PMID: 31320251
-
Immunoglobulin A Deposits In Renal Allografts: A Prospective Longitudinal Single-Center Study.Transplant Proc. 2024 Jan-Feb;56(1):97-104. doi: 10.1016/j.transproceed.2023.11.023. Epub 2024 Jan 12. Transplant Proc. 2024. PMID: 38216361
-
Oxford Classification of IgA nephropathy 2016: an update from the IgA Nephropathy Classification Working Group.Kidney Int. 2017 May;91(5):1014-1021. doi: 10.1016/j.kint.2017.02.003. Epub 2017 Mar 22. Kidney Int. 2017. PMID: 28341274 Review.
-
Pediatric IgA Nephropathy in Europe.Kidney Dis (Basel). 2019 Jun;5(3):182-188. doi: 10.1159/000495751. Epub 2019 Jan 24. Kidney Dis (Basel). 2019. PMID: 31259180 Free PMC article. Review.
Cited by
-
The role of zinc in follicular development.Mol Biol Rep. 2023 May;50(5):4527-4534. doi: 10.1007/s11033-023-08331-6. Epub 2023 Feb 27. Mol Biol Rep. 2023. PMID: 36848006 Review.
-
Urinary exosomal miRNA-451a can be used as a potential noninvasive biomarker for diagnosis, reflecting tubulointerstitial damage and therapeutic response in IgA nephropathy.Ren Fail. 2024 Dec;46(1):2319326. doi: 10.1080/0886022X.2024.2319326. Epub 2024 Feb 20. Ren Fail. 2024. PMID: 38379319 Free PMC article.
References
-
- Working Group of the International IgA Nephropathy Network and the Renal Pathology Society. Cattran DC, Coppo R, Cook HT, Feehally J, Roberts ISD, et al. . The Oxford classification of IgA nephropathy: Rationale, clinicopathological correlations, and classification. Kidney Int (2009) 76(5):534–45. doi: 10.1038/ki.2009.243 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous