

A rare case of multiple paragangliomas in the head and neck, retroperitoneum and duodenum: A case report and review of the literature
- PMID: 36704041
- PMCID: PMC9871575
- DOI: 10.3389/fendo.2022.1054468
A rare case of multiple paragangliomas in the head and neck, retroperitoneum and duodenum: A case report and review of the literature
Abstract
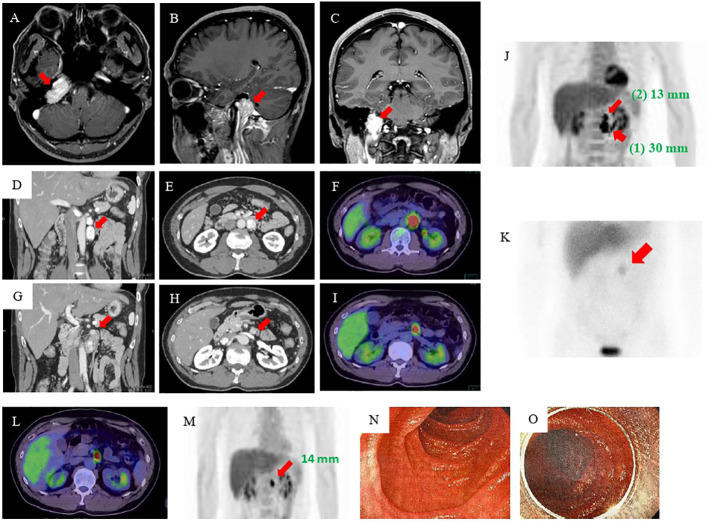
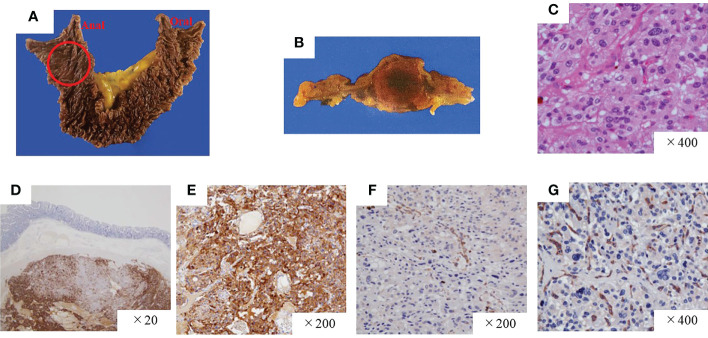
Pheochromocytomas and paragangliomas (PGLs) are rare non-epithelial neuroendocrine neoplasms of the adrenal medulla and extra-adrenal paraganglia respectively. Duodenal PGL is quite rare and there are only two previous reports. Herein, we report a case of multiple catecholamines (CAs)-producing PGLs in the middle ear, retroperitoneum, and duodenum, and review the literature of duodenal PGLs. A 40-year-old man complained right-ear hearing loss, and an intracranial tumor was suspected. Magnetic resonance imaging of the head revealed a 3-cm mass at the right transvenous foramen, which was surgically resected following preoperative embolization. The pathological diagnosis was a sympathetic PGL of the right middle ear. Six years later, family history of PGL with germline mutation of succinate dehydrogenase complex iron sulfur subunit B, SDHB: c.268C>T (p.Arg90Ter) was clarified. The patient had elevated levels of plasma and urine CAs again. Abdominal computed tomography scanning revealed two retroperitoneal tumors measuring 30-mm at the anterior left renal vein and 13-mm at near the ligament of Treitz. The larger tumor was laparoscopically resected, but the smaller tumor was not identified by laparoscopy. After the operation, the patient remained hypertensive, and additional imaging tests suggested a tumor localized in the duodenum. The surgically resected tumor was confirmed to be a duodenal PGL. After that, the patient remained hypertension free, and urinary levels of noradrenaline and normetanephrine decreased to normal values. No recurrence or metastasis has been found at 1 year after the second operation. CAs secretion from PGLs in unexpected location, like the duodenum of our patient, may be overlooked and leads to a hypertensive crisis. In such cases, comprehensive evaluation including genetic testing, fluorodeoxyglucose-positron emission tomography scanning, and measurement of CAs will be useful for detecting PGLs. Most previous reports on duodenal PGL were gangliocytic PGL which has been renamed composite gangliocytoma/neuroma and neuroendocrine tumor, and defined the different tumor from duodenal PGL. We reviewed and discussed duodenal PGLs in addition to multiple PGLs associated with SDHB mutation.
Keywords: catecholamine-secreting tumor; duodenal paraganglioma; head and neck paraganglioma (HNPGL); hereditary paraganglioma; multiple paragangliomas; succinate dehydrogenase B mutation.
Copyright © 2023 Kawanabe, Katabami, Oshima, Yanagisawa, Sone and Kimura.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Clinical aspects of SDHx-related pheochromocytoma and paraganglioma.Endocr Relat Cancer. 2009 Jun;16(2):391-400. doi: 10.1677/ERC-08-0284. Epub 2009 Feb 3. Endocr Relat Cancer. 2009. PMID: 19190077 Free PMC article. Review.
-
Clinical presentations, biochemical phenotypes, and genotype-phenotype correlations in patients with succinate dehydrogenase subunit B-associated pheochromocytomas and paragangliomas.J Clin Endocrinol Metab. 2007 Mar;92(3):779-86. doi: 10.1210/jc.2006-2315. Epub 2007 Jan 2. J Clin Endocrinol Metab. 2007. PMID: 17200167
-
Colorectal paragangliomas with immunohistochemical deficiency of succinate dehydrogenase subunit B.Endocr J. 2022 May 30;69(5):523-528. doi: 10.1507/endocrj.EJ21-0630. Epub 2021 Dec 1. Endocr J. 2022. PMID: 34853215
-
Biochemically silent abdominal paragangliomas in patients with mutations in the succinate dehydrogenase subunit B gene.J Clin Endocrinol Metab. 2008 Dec;93(12):4826-32. doi: 10.1210/jc.2008-1093. Epub 2008 Oct 7. J Clin Endocrinol Metab. 2008. PMID: 18840642 Free PMC article.
-
Overview of the 2022 WHO Classification of Paragangliomas and Pheochromocytomas.Endocr Pathol. 2022 Mar;33(1):90-114. doi: 10.1007/s12022-022-09704-6. Epub 2022 Mar 13. Endocr Pathol. 2022. PMID: 35285002 Review.
Cited by
-
Left Renal Vein Transection and Reconstruction for Functional Paraganglioma Resection: A Case Report.Vasc Specialist Int. 2025 Jun 25;41:14. doi: 10.5758/vsi.250017. Vasc Specialist Int. 2025. PMID: 40556353 Free PMC article.
-
Case Report: A 65-year-old man with paraganglioma accompanied by elevated interleukin-6 levels and KIF1B single gene mutation.Front Endocrinol (Lausanne). 2023 Sep 14;14:1226468. doi: 10.3389/fendo.2023.1226468. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37780619 Free PMC article.
-
Subclinical paraganglioma of the retroperitoneum: A case report.World J Clin Cases. 2024 May 26;12(15):2672-2677. doi: 10.12998/wjcc.v12.i15.2672. World J Clin Cases. 2024. PMID: 38817224 Free PMC article.
-
Multiple Primary Paragangliomas in a Pediatric Patient With von Hippel Lindau: A Diagnostic Dilemma.JCEM Case Rep. 2024 Sep 9;2(9):luae160. doi: 10.1210/jcemcr/luae160. eCollection 2024 Sep. JCEM Case Rep. 2024. PMID: 39253568 Free PMC article.
-
Gastric paraganglioma: a case report and review of literature.Front Oncol. 2024 Apr 2;14:1357612. doi: 10.3389/fonc.2024.1357612. eCollection 2024. Front Oncol. 2024. PMID: 38628664 Free PMC article.
References
-
- Garcia-Carbonero R, Matute Teresa F, Mercader-Cidoncha E, Mitjavila-Casanovas M, Robledo M, Tena I, et al. . Multidisciplinary practice guidelines for the diagnosis, genetic counseling and treatment of pheochromocytomas and paragangliomas. Clin Transl Oncol (2021) 23(10):1995–2019. doi: 10.1007/s12094-021-02622- - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous